Epidemiology is the foundational science of public health, providing the methods and evidence needed to understand the distribution and determinants of health-related events in populations. Through systematic data collection, analysis, and interpretation, epidemiology supports informed decision-making aimed at preventing disease, reducing health disparities, and improving population health outcomes. The discipline performs several core functions that collectively enable effective public health action and health system planning.
One of the primary epidemiologic functions is public health surveillance. Public health surveillance involves the continuous and systematic collection, analysis, interpretation, and dissemination of health data. Surveillance systems monitor disease occurrence, detect unusual health events, identify emerging threats, and provide information necessary for timely interventions. These systems serve as an early warning mechanism for outbreaks and other public health emergencies.
A second key function is the investigation of disease outbreaks and health events. Epidemiologists identify the source, mode of transmission, and risk factors associated with outbreaks, enabling rapid implementation of control measures. Outbreak investigations are critical for limiting disease spread and protecting vulnerable populations.
Another essential function is the identification of risk factors and determinants of health. Epidemiologic studies examine the relationships between exposures and health outcomes to determine factors that increase or decrease disease risk. These determinants may include biological, environmental, behavioral, social, and occupational influences. Understanding such factors helps guide prevention strategies and health promotion programs.
Epidemiology also plays a central role in the evaluation of public health interventions, policies, and programs. By assessing the effectiveness, efficiency, and impact of interventions, epidemiologists generate evidence that supports resource allocation and policy development. Evaluation findings help refine existing programs and inform future public health initiatives. Epidemiology contributes to evidence-based decision-making and health planning. Epidemiologic evidence informs clinical guidelines, public health policies, and resource prioritization at local, national, and global levels. These core functions provide the scientific framework necessary for disease prevention, health protection, and the advancement of population health.
Evolution of epidemiologys five core tasks and the emergence of policy development
In the mid-1980s, epidemiology’s role in public health practice was formalized into a structured framework of core functions aimed at defining how epidemiologic science is operationalized within real-world public health systems. This development reflected a broader shift in the discipline from a primarily descriptive and academic pursuit toward an applied science directly embedded in decision-making, program implementation, and population health improvement. The intent was to provide a coherent conceptual map of what epidemiologists actually do in practice and how their activities collectively support the prevention and control of disease at the population level.
The resulting framework originally articulated five major tasks that define the operational scope of applied epidemiology: public health surveillance, field investigation, analytic studies, evaluation, and linkage. Although presented as distinct categories for clarity, these tasks function in practice as an integrated system of activities that are continuously interacting. Together, they describe the full lifecycle of epidemiologic work from the generation of health data to its interpretation, application, and dissemination across public health systems.
At a structural level, this framework was developed to standardize epidemiologic practice across diverse public health institutions and jurisdictions. Prior to its formal articulation, epidemiologic activities were often dispersed across different programs and agencies without a unified conceptual structure, resulting in inconsistencies in how data were collected, interpreted, and translated into action. The mid-1980s formulation addressed this gap by explicitly linking epidemiologic methods to public health functions, ensuring that surveillance data could inform investigation, that analytical findings could guide intervention, and that programmatic outcomes could be systematically assessed. In this sense, the framework is both descriptive, capturing what epidemiologists do and normative, defining what they should do within an effective public health system.
Within this system, each of the five tasks occupies a specific functional role. Public health surveillance is responsible for the continuous collection, analysis, and interpretation of health-related data for the purposes of monitoring population health and detecting changes in disease patterns. Field investigation focuses on the rapid response to unusual health events, including outbreaks and clusters, with the aim of confirming diagnoses, identifying sources, and implementing immediate control measures. Analytic studies provide the methodological foundation for testing hypotheses about determinants of health and disease using structured epidemiologic designs such as cohort, case-control, and cross-sectional studies. Evaluation examines the effectiveness, efficiency, and impact of public health programs and interventions, ensuring accountability and guiding improvements in program design and implementation. Linkage refers to the coordination and integration of epidemiologic data and expertise across agencies, laboratories, healthcare systems, and policy institutions to ensure that information is translated into coherent public health action.
These five tasks form a dynamic and iterative system in which information flows between observation, analysis, and intervention. Surveillance generates signals that may trigger field investigations; findings from investigations may lead to analytic studies for confirmation; results from analytic work inform interventions that are subsequently evaluated; and linkage ensures that all components are coordinated across institutional boundaries. This interconnected structure highlights the systems-oriented nature of epidemiology as a discipline operating at the interface of science and public health practice.
In subsequent expansions of this framework, a sixth task, policy development was added as a major function of epidemiology in public health practice. This addition reflects the increasing recognition that epidemiologic evidence does not only inform scientific understanding or programmatic action but also plays a central role in shaping formal public health policies, regulations, and legislative decisions. Policy development involves the translation of epidemiologic findings into actionable guidance, standards, and rules that govern population health interventions at local, national, and international levels. The inclusion of this sixth task underscores the evolving role of epidemiology as not only an analytical and evaluative discipline but also a foundational input into governance and structured decision-making processes in public health systems.
Public health surveillance
Public health surveillance is defined as the ongoing, systematic collection, analysis, interpretation, and dissemination of health-related data for use in planning, implementing, and evaluating public health practice. It is a foundational function of epidemiology and is often described as the “information system for action” because its primary purpose is not merely data accumulation, but the timely production of actionable intelligence that supports disease prevention and control. Conceptually, surveillance can be understood as the continuous monitoring of the health status of populations analogous to tracking the physiological “pulse” of a community to detect deviations from expected patterns that may signal emerging health threats, changes in disease burden, or the impact of interventions.
At its core, surveillance operates through a structured cycle. Data are first collected from multiple sources, then systematically analyzed to identify patterns, interpreted in the context of population health, and finally disseminated to stakeholders responsible for public health decision-making. This process ensures that information flows efficiently from data generators to decision-makers, enabling timely interventions. Importantly, surveillance is not a passive activity; it is an organized system designed to trigger action when necessary and to provide continuous feedback on the state of public health.
A central component of traditional surveillance systems is the reporting of morbidity and mortality data. Local and state health departments routinely receive case reports of notifiable diseases from healthcare providers, infection prevention specialists, and clinical laboratories. These reporting systems are often mandated by law and require the notification of specific conditions such as pertussis, meningococcal meningitis, measles, tuberculosis, or human immunodeficiency virus (HIV) infection. Mortality data, typically derived from death certificates, complement morbidity reporting by providing insight into disease severity, case fatality, and long-term population health outcomes. Together, morbidity and mortality reports form the backbone of many surveillance systems and provide essential baseline information for monitoring disease trends.
Beyond routine reporting systems, surveillance draws on a wide range of supplementary data sources that enhance completeness and improve interpretability. These include detailed investigations of individual cases and outbreak clusters, which provide contextual information about transmission dynamics and risk factors. Public health program data, such as immunization coverage rates, screening uptake, and treatment adherence metrics, are also critical for evaluating the performance of prevention programs. Disease registries such as cancer registries or congenital anomaly registries offer structured, long-term datasets that enable tracking of incidence, survival, and disease progression. In addition, population-based health surveys provide self-reported or measured data on risk factors, health behaviors, and access to healthcare, allowing surveillance systems to capture conditions that may not be clinically diagnosed or reported.
In most practical settings, surveillance systems rely on relatively simple and standardized reporting mechanisms that collect a limited set of essential variables for each case, such as demographic characteristics, diagnosis, date of onset, and geographic location. Although underreporting is a recognized limitation since not every case of disease is captured surveillance systems are designed to function effectively even with incomplete data. Epidemiologists compensate for these limitations by focusing on trends, patterns, and relative changes over time rather than absolute counts alone. Regular review of incoming data allows health officials to detect unusual increases in disease frequency, geographic clustering of cases, or shifts in population distribution that may warrant further investigation or intervention.
Historically, surveillance systems were primarily focused on communicable diseases, particularly those with outbreak potential or high public health impact. However, the scope of surveillance has expanded substantially over time to include non-communicable diseases such as cardiovascular disease, cancer, diabetes, and chronic respiratory conditions. In addition, modern surveillance systems increasingly incorporate injury surveillance, occupational health monitoring, environmental exposure tracking, genetic and congenital disorder registries, and behavioral risk factor surveillance. This expansion reflects the broadening mandate of public health to address the full spectrum of determinants affecting population health, including environmental, occupational, genetic, and lifestyle-related factors.
A major transformation in surveillance practice occurred in the early 21st century, particularly following the events of September 11, 2001, which highlighted the need for rapid detection of bioterrorism threats and emerging infectious diseases. This led to the development and widespread implementation of syndromic and electronic surveillance systems. These systems leverage real-time or near-real-time data sources such as emergency department chief complaints, over-the-counter pharmaceutical sales, school or workplace absenteeism records, and electronic health records. By capturing early indicators of illness before formal diagnosis, syndromic surveillance enhances the timeliness of detection and allows for earlier public health response.
As surveillance systems have become more technologically advanced, the role of the epidemiologist has also evolved. Modern surveillance practice requires strong competencies in data management, statistical analysis, and data visualization, as well as the ability to design data collection instruments and ensure data quality. Epidemiologists must also be skilled in interpreting complex datasets, identifying meaningful epidemiologic signals within large volumes of information, and communicating findings clearly through scientific reports, presentations, and policy briefs. These skills are essential for translating raw data into actionable public health intelligence.
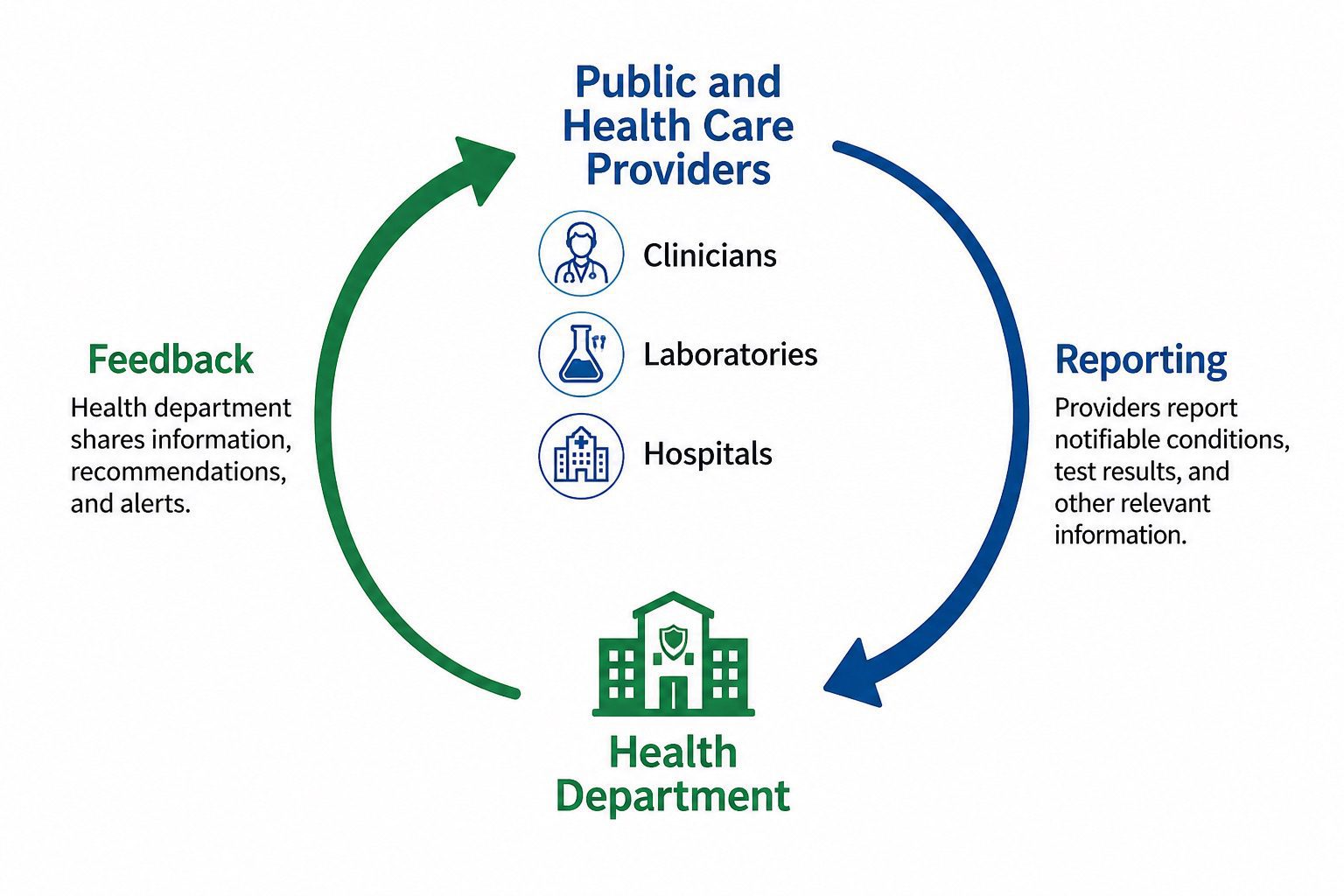
Surveillance is not a unidirectional process. An essential feature of effective surveillance systems is feedback. Information generated by health departments is routinely communicated back to clinicians, laboratories, hospitals, and other reporting entities (Figure 2). This feedback loop reinforces participation in surveillance systems, improves data quality, and ensures that frontline healthcare providers remain informed about current disease trends and public health priorities. In this way, surveillance functions as a dynamic, interconnected system that supports continuous learning, accountability, and evidence-based decision-making across the entire public health infrastructure.
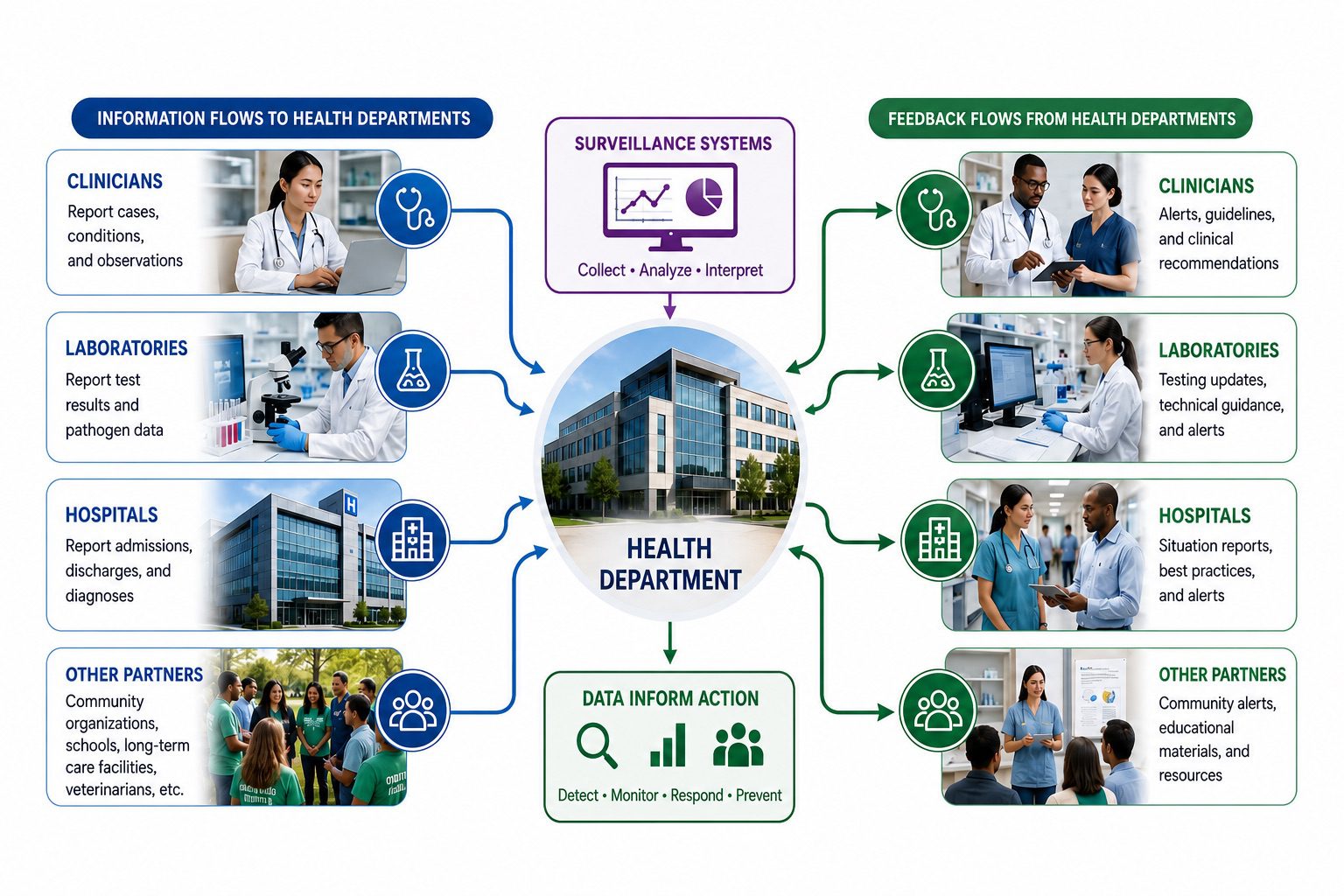
Figure 2. Public health surveillance information flow between healthcare providers and health departments. Surveillance data are reported from healthcare providers and community partners, including clinicians, laboratories, hospitals, and other stakeholders, to health departments for collection, analysis, interpretation, and action. Health departments subsequently provide feedback, alerts, guidelines, technical recommendations, situation reports, and educational resources to reporting entities, creating a continuous bidirectional communication system that supports disease monitoring, outbreak detection, prevention, and public health response.
Field investigation
Field investigation is a central operational component of applied epidemiology and represents the immediate, action-oriented response that follows the detection of unusual health events through surveillance systems. As surveillance provides structured information for identifying potential public health threats, field investigation constitutes the first substantive step in transforming that information into targeted inquiry and intervention. The triggering signal may originate from a routine surveillance case report, an alert from a clinician, a laboratory notification, or the detection of a disease cluster that exceeds expected baseline levels. Once such a signal is identified, public health authorities initiate an investigation whose scope is determined by the severity, transmissibility, and uncertainty surrounding the event.
The scale and complexity of field investigations vary considerably. In some instances, the investigative response is relatively limited and may involve a simple telephone call or electronic communication with the reporting healthcare provider to verify diagnostic details, confirm clinical findings, or clarify exposure history. In other situations, particularly during outbreaks or rapidly evolving epidemics, the response escalates into a large, coordinated field operation involving multidisciplinary teams of epidemiologists, laboratorians, infection control specialists, environmental health officers, and sometimes law enforcement or regulatory agencies. These large-scale investigations may span multiple jurisdictions and require systematic case finding, extensive data collection, environmental assessments, and real-time data analysis to characterize the extent of transmission and identify its underlying cause.
The objectives of field investigations are diverse and context-dependent, but they consistently revolve around interrupting transmission, identifying sources of infection, and generating actionable epidemiologic intelligence.One of the most immediate and frequently encountered objectives is the identification of additional cases that have not yet been reported or recognized by the healthcare system. These undetected cases are epidemiologically important because they may continue to transmit infection within the community. Early detection and isolation of such individuals is therefore a key mechanism for controlling outbreaks.
This objective is particularly evident in investigations of sexually transmitted infections (STIs), where contact tracing is a core investigative tool. In these settings, epidemiologists and disease intervention specialists systematically interview infected individuals to identify sexual partners or close contacts who may have been exposed. Many of these contacts are asymptomatic at the time of identification, yet laboratory testing often reveals active infection. Prompt treatment of these individuals not only benefits their individual health outcomes but also serves as a critical intervention for breaking chains of transmission within sexual networks. This approach demonstrates how field investigation directly integrates epidemiologic reasoning with preventive action at the population level.
In other outbreak scenarios, field investigations are designed to identify the specific source or vehicle of infection, particularly when transmission is linked to contaminated food, water, or environmental exposure. A classic example involves infections caused by Escherichia coli O157:H7, a pathogen frequently associated with foodborne outbreaks. Investigations typically focus on reconstructing exposure histories among affected individuals to identify common food items consumed prior to illness onset. Ground beef is a well-documented vehicle, although outbreaks have also been linked to produce, unpasteurized juices, and other less typical sources. Once a likely vehicle is identified, investigators can assess the distribution of exposure, estimate the population at risk, and determine whether contamination occurred at the production, processing, or retail level.
When a commercial product is implicated as the source of infection, field investigations can lead to rapid public health interventions such as product recalls, public advisories, and regulatory enforcement actions. These measures are designed to prevent additional exposures and reduce the overall burden of disease in the population. The effectiveness of such interventions depends heavily on the speed and accuracy of the investigative process, underscoring the importance of timely data collection, laboratory confirmation, and interagency coordination.
In some instances, the primary objective of a field investigation is not immediate control but rather the generation of foundational knowledge about a disease that is not yet well understood. This is often the case during the emergence of novel pathogens or previously unrecognized syndromes. Early investigations of the 2003 severe acute respiratory syndrome (SARS) outbreak exemplify this function. At the outset, epidemiologists lacked a standardized case definition, and there was limited understanding of transmission dynamics, incubation periods, and risk factors. Field investigations during this period focused on systematically describing cases in terms of time, place, and person, thereby establishing the descriptive epidemiology necessary for further analytical work. As evidence accumulated, more refined recommendations regarding infection control, isolation procedures, and quarantine measures were developed and implemented.
Field investigations of this nature are often colloquially referred to as “shoe leather epidemiology,” a term that reflects the intensive, hands-on nature of the work. It evokes the image of epidemiologists physically traveling to hospitals, communities, laboratories, and affected sites to collect data, interview patients, and observe environmental conditions firsthand. This approach emphasizes direct engagement with real-world conditions rather than reliance solely on secondary data sources. The term has become emblematic of applied epidemiology’s pragmatic and investigative ethos. The importance of this tradition is symbolically captured in the emblem of the Epidemic Intelligence Service (EIS), the Centers for Disease Control and Prevention’s (CDC) elite training program for field epidemiologists. The symbol, a shoe with a hole in the sole, represents the extensive fieldwork and physical mobility required of disease detectives who must rapidly respond to public health threats wherever they emerge. This imagery reinforces the enduring role of field investigation as a cornerstone of epidemiologic practice, one that bridges surveillance data and actionable public health intervention through direct, evidence-driven inquiry.
Analytic studies
While surveillance and field investigations often identify disease causes and guide control measures, some situations require more rigorous scientific evaluation. In these cases, epidemiologists conduct analytic studies to test hypotheses and determine whether observed associations between exposures and health outcomes are likely to be causal. Analytic epidemiology provides the scientific evidence needed to support effective public health interventions, policies, and programs. Analytic studies are usually integrated with surveillance and field investigations. Surveillance systems detect unusual disease patterns or outbreaks, while field investigations provide preliminary information about affected populations and potential exposures. Together, these activities generate hypotheses that can be formally tested through analytic studies, linking observation to evidence-based decision-making.
Disease investigations often begin with descriptive epidemiology, which examines disease distribution by time, place, and person. Descriptive analyses help identify populations at risk and reveal patterns that may suggest possible causes. Although some associations are sufficiently obvious to guide action, most descriptive findings generate hypotheses that require analytic evaluation. The defining feature of analytic epidemiology is the use of a comparison group. By comparing exposed and unexposed individuals, or diseased and non-diseased populations, epidemiologists assess whether an association exists between exposure and outcome. Common study designs include cohort, case-control, and cross-sectional studies. The validity of findings depends heavily on selecting an appropriate comparison group.
Analytic studies require careful planning, including choosing a study design, defining eligibility criteria, determining sample size, developing data collection tools, and establishing quality assurance procedures. Implementation involves obtaining ethical approvals, recruiting participants, collecting epidemiologic and laboratory data, and ensuring data accuracy and confidentiality. Data analysis begins with describing the study population and then quantifying associations using measures such as risk ratios, prevalence ratios, and odds ratios. More advanced methods may address confounding and complex relationships among variables. Epidemiologists interpret findings by considering biological plausibility, bias, limitations, and public health significance. By rigorously testing hypotheses, analytic studies provide the foundation for identifying risk factors, understanding disease causation, evaluating interventions, and guiding evidence-based public health action.
Evaluation
Evaluation is a core function of public health practice and applied epidemiology. As public health programs and interventions have become more complex and resource-intensive, the need for systematic assessment has increased. Epidemiologists play a central role in evaluation by applying scientific methods and data analysis to determine whether programs achieve their intended goals, use resources appropriately, and improve population health. Evaluation is the systematic and objective assessment of a program’s design, implementation, performance, and outcomes. It examines relevance, effectiveness, efficiency, impact, and sustainability, providing evidence for decision-making, accountability, quality improvement, and future planning. Through evaluation, strengths and weaknesses can be identified, allowing programs to be refined and optimized.
A key component of evaluation is effectiveness, which measures the extent to which a program achieves its objectives under real-world conditions. This differs from efficacy, which refers to performance under ideal or controlled settings. While efficacy demonstrates potential, effectiveness reflects actual public health impact in routine practice. Efficiencyassesses whether desired outcomes are achieved with optimal use of resources such as time, personnel, and funding. Because public health resources are often limited, efficiency evaluations help guide resource allocation and program sustainability. Evaluation may occur at different stages of a program. Formative evaluation is conducted during planning or early implementation to improve program design and identify potential barriers. Process evaluation examines whether activities are implemented as intended, focusing on coverage, service delivery, protocol adherence, and resource use. Impact or summative evaluation assesses immediate and intermediate effects of an intervention, while outcome evaluation focuses on long-term changes in health status, disease burden, behavior, or quality of life.
For example, evaluation of an immunization program may assess vaccine coverage, delivery efficiency, and reductions in disease incidence. Similarly, surveillance system evaluations examine attributes such as data quality, timeliness, sensitivity, and usefulness. Evaluation provides essential evidence to improve programs, strengthen public health systems, ensure accountability, and enhance population health outcomes.
Linkages
A defining characteristic of public health epidemiology is its collaborative nature. Epidemiologists rarely work in isolation, particularly when addressing complex health challenges involving multiple determinants and stakeholders. Linkages refer to the professional relationships, communication channels, partnerships, and networks that connect epidemiologic knowledge to the broader public health system. These linkages enable information exchange, coordination of activities, and the translation of scientific findings into effective public health action. The importance of linkages arises from the multidisciplinary nature of public health. Disease prevention and control require contributions from medicine, microbiology, environmental health, nursing, biostatistics, health informatics, social sciences, and policy. Consequently, epidemiologists work within networks of professionals whose collective expertise supports the identification, investigation, and management of health problems. This collaborative environment has led many practitioners to describe field epidemiology as a “team sport.”
During outbreak investigations and public health emergencies, epidemiologists often participate in multidisciplinary teams that may include laboratorians, clinicians, nurses, infection prevention specialists, environmental health professionals, communication experts, and information technology specialists. Integrating these diverse perspectives improves the efficiency and effectiveness of epidemiologic investigations. Linkages are particularly important because many public health problems cross organizational and geographic boundaries. Infectious disease outbreaks, environmental exposures, and other emerging threats often require collaboration among local, national, and international agencies, as well as academic institutions, healthcare organizations, and non-governmental partners. These partnerships provide access to expertise, surveillance data, laboratory resources, and logistical support.
Beyond emergencies, linkages support routine activities such as disease surveillance, program evaluation, health promotion, and policy implementation. Effective collaboration improves disease reporting, diagnostic confirmation, information dissemination, and community engagement. Both formal mechanisms, such as data-sharing agreements and joint training programs, and informal professional networks strengthen these connections. Linkages highlight that epidemiology is not only a scientific discipline but also a collaborative enterprise. By fostering communication, coordination, and cooperation, linkages enhance the ability of public health systems to prevent disease, protect communities, and improve population health.
Policy development
Policy development is a core function of modern epidemiology because it connects scientific evidence with public health action. Epidemiology is traditionally defined as the study of the distribution and determinants of health-related events and the application of this knowledge to control health problems. This application component highlights the importance of translating research findings into policies that improve population health. Historically, some epidemiologists, particularly in academic settings, argued that their role should be limited to generating and analyzing evidence, leaving policy decisions to others. Although this perspective emphasizes scientific objectivity, it is often impractical in public health practice. Epidemiologists working in government and public health agencies frequently face urgent health threats that require immediate decisions regarding prevention, control, and resource allocation. In such situations, evidence must be translated into action.
Public health epidemiologists are well positioned to contribute to policy development because of their expertise in disease patterns, risk factors, vulnerable populations, and intervention effectiveness. Through surveillance, outbreak investigations, analytic studies, and program evaluations, they generate knowledge that helps identify priority health issues and assess the likely impact of interventions. Their recommendations ensure that policies are informed by scientific evidence rather than assumptions or anecdotal observations. Policy development includes activities such as advising government officials, contributing to public health regulations, serving on advisory committees, and preparing reports that guide legislative and administrative decisions. Epidemiologists also help develop guidelines and standards related to vaccination programs, infectious disease control, environmental health, antimicrobial resistance, and chronic disease prevention.
Effective policy development requires consideration of economic, social, and ethical factors. Epidemiologists support decision-making by quantifying disease burden, identifying high-risk populations, evaluating interventions, and assessing potential consequences of policy actions. After implementation, they continue to monitor and evaluate outcomes, providing evidence for policy refinement. Thus, policy development is a continuous process that links scientific inquiry, decision-making, implementation, and evaluation to improve population health.
Source
Aschengrau, A., & G. R. Seage III. (2009). Essentials of Epidemiology in Public Health. Boston: Jones and Bartlett Publishers.
Balows A, Hausler W, Herrmann K.L, Isenberg H.D and Shadomy H.J (1991). Manual of clinical microbiology. 5th ed. American Society of Microbiology Press, USA.
Bonita R., Beaglehole R., Kjellström T (2006). Basic epidemiology. 2nd edition. World Health Organization. Pp. 1-226.
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA.
Castillo-Salgado C (2010). Trends and directions of global public health surveillance. Epidemiol Rev, 32:93–109.
Center for Disease Control and Prevention (CDC)
Porta M (2008). A dictionary of epidemiology. 5th edition. New York: Oxford University Press.
Rothman K.J and Greenland S (1998). Modern epidemiology, 2nd edition. Philadelphia: Lippincott-Raven.
Rothman K.J, Greenland S and Lash T.L (2011). Modern Epidemiology. Third edition. Lippincott Williams and Wilkins, Philadelphia, PA, USA.
www.cdc.gov/csels/dsepd/ss1978/lesson1/section4.html
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.