Epidemiological studies are a foundational component of public health research, providing systematic methods to investigate the distribution, determinants, and dynamics of health-related states and events in defined populations. The aim of epidemiological studies is to answer three central questions: who is affected, where and when the outcomes occur, and why they occur. By linking exposures to outcomes in human populations, epidemiology informs disease prevention strategies, guides clinical practice, and supports evidence-based policy development.
The field is broadly divided into descriptive and analytical epidemiology. Descriptive epidemiology focuses on characterizing health events in terms of person, place, and time. It establishes patterns of disease occurrence and generates hypotheses about potential causal factors. For example, describing the incidence of infectious diseases across different age groups or geographic regions can reveal vulnerable populations or environmental risk factors. Measures commonly used in descriptive studies include incidence, prevalence, and mortality rates, which collectively provide a snapshot of disease burden.
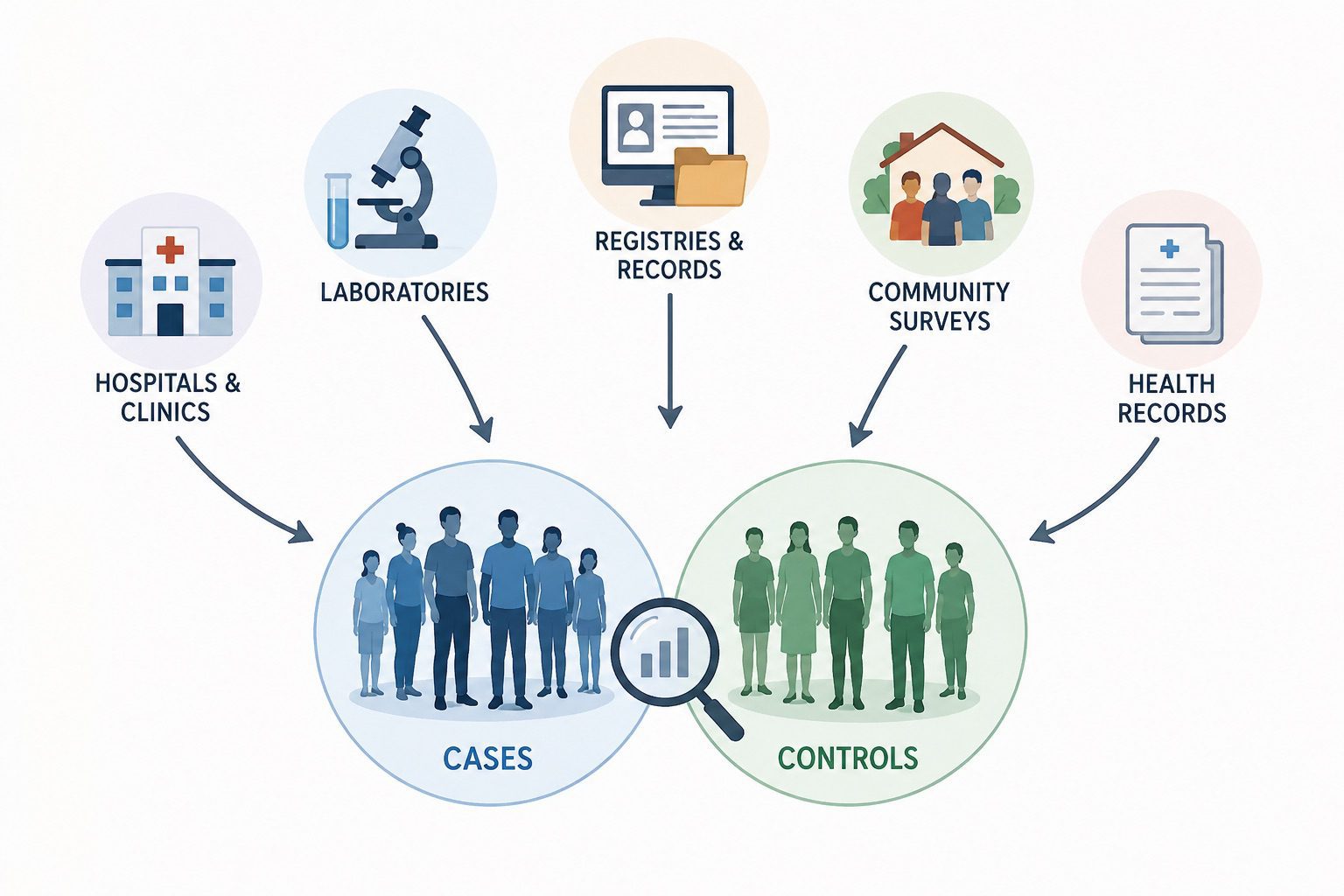
Analytical epidemiology, on the other hand, is concerned with testing hypotheses about causal relationships between exposures and outcomes. It typically involves comparison groups to evaluate whether specific exposures are associated with increased or decreased risk of disease. Analytical studies are further classified into observational and experimental designs. Observational studies include cohort, case-control, and cross-sectional designs. Cohort studies follow exposed and unexposed individuals over time to assess the development of outcomes, allowing direct estimation of risk and temporal relationships. Case-control studies, on the other hand, compare individuals with a disease (cases) to those without (controls) to retrospectively assess exposure history, making them particularly efficient for rare diseases. Cross-sectional studies assess exposure and outcome simultaneously, providing prevalence estimates but limited causal inference due to the lack of temporality.
Experimental epidemiology, often represented by randomized controlled trials (RCTs), involves deliberate assignment of exposures or interventions by the investigator. Randomization reduces confounding and bias, making RCTs the gold standard for evaluating intervention efficacy. However, ethical, financial, and logistical constraints often limit their use, especially in population-level or long-term exposure studies.
A critical aspect of epidemiological research is the assessment and control of bias and confounding. Bias refers to systematic errors in study design or execution that distort the true association between exposure and outcome. Common types include selection bias, information bias, and recall bias. Confounding occurs when an extraneous variable is associated with both the exposure and outcome, potentially leading to a spurious association. Techniques such as randomization, restriction, matching, and multivariable statistical adjustment are employed to minimize these issues.
Epidemiological studies also rely heavily on measures of association to quantify relationships between exposures and outcomes. These include risk ratios, odds ratios, and hazard ratios, each appropriate for different study designs and data structures. Interpretation of these measures requires careful consideration of confidence intervals and statistical significance, as well as biological plausibility.
In modern public health, epidemiology extends beyond infectious disease surveillance to include chronic diseases, environmental exposures, occupational hazards, and emerging global health threats. It plays a central role in understanding complex conditions such as cancer, cardiovascular disease, and antimicrobial resistance, where multiple interacting risk factors are involved. Advances in computational methods, large-scale cohort studies, and genomic epidemiology have further expanded the field’s capacity to identify subtle associations and causal pathways. Epidemiological studies provide the empirical foundation for understanding health patterns and informing interventions at both individual and population levels. Their strength lies in their ability to integrate statistical rigor with real-world complexity, making them indispensable for advancing global health outcomes.
Formulating the hypothesis and defining the epidemiological question
An epidemiological study is typically structured around a systematic process that begins with two critical preparatory steps, both of which are essential before any meaningful investigation of a disease or infection outbreak can commence. The first and most fundamental step is the formulation of a clear, testable hypothesis. In epidemiological terms, a hypothesis is a structured statement that proposes a potential relationship between an exposure (or set of exposures) and a health-related outcome. This hypothesis provides the conceptual backbone of the entire investigation and determines the direction of data collection, analysis, and interpretation.
A well-defined epidemiological hypothesis must explicitly describe both the exposure and the expected outcome. The exposure may include biological agents such as pathogens, environmental factors such as contaminated water or air pollutants, behavioural determinants such as smoking or dietary habits, or healthcare-related factors such as antibiotic use or vaccination status. The outcome, on the other hand, refers to the disease or health event of interest, such as infection, morbidity, mortality, or a measurable physiological condition. Importantly, a strong hypothesis also considers the population under investigation, ensuring clarity regarding who is at risk and under what contextual conditions the exposure–outcome relationship is expected to occur.
The formulation of a hypothesis is not merely a theoretical exercise; it is grounded in preliminary observations, surveillance data, previous research findings, or field reports from outbreak settings. In outbreak investigations, for instance, descriptive epidemiology often provides the first clues regarding potential sources and transmission routes, which are then translated into analytic hypotheses. This transition from observation to hypothesis is critical, as it transforms raw epidemiological signals into structured research questions that can be empirically tested.
In addition, hypothesis formulation serves as a guiding framework for determining what data are necessary, what comparisons are meaningful, and what statistical methods are appropriate. Without a clearly articulated hypothesis, epidemiological investigations risk becoming unfocused, inefficient, or prone to misinterpretation. Therefore, the precision and clarity of the hypothesis directly influence the validity and reliability of the entire study.
Selection of study design and considerations in epidemiological investigation
The second essential step in any epidemiological investigation is the selection of an appropriate study design to test the predefined hypothesis. This decision is a central methodological consideration and must be made with careful attention to the nature of the research question, available resources, ethical constraints, and the expected validity of the findings. The choice of study design ultimately determines how data are collected, how associations are measured, and how confidently conclusions can be drawn.
Epidemiological study designs are broadly diverse, reflecting the multiple ways in which health-related information can be gathered, structured, and interpreted in the context of disease occurrence. Each design has specific strengths and limitations, and no single approach is universally superior. Instead, the appropriateness of a design depends on the epidemiological context and the specific objectives of the investigation.
Broadly, epidemiological investigations can be directed toward two main objectives: identifying the determinants of disease or describing the patterns of disease distribution within a defined population. Descriptive studies focus on characterizing disease occurrence by person, place, and time, thereby providing essential baseline information about the burden and spread of disease. Analytical studies, in contrast, aim to test hypotheses by examining relationships between exposures and outcomes, often through comparison groups. Together, these approaches form the backbone of epidemiological reasoning, allowing investigators to move from observation to causal inference.
The variety of available study designs reflects different methodological strategies for obtaining epidemiological data during disease or infection outbreaks. These include observational designs such as cross-sectional, case-control, and cohort studies, as well as experimental designs such as randomized controlled trials. Each design differs in how exposure is assigned or measured, the directionality of data collection, and the strength of causal inference it can support. For example, cohort studies are particularly useful for examining incidence and temporal relationships, while case-control studies are efficient for rare diseases or outbreaks with limited time frames. Experimental studies, although less common in outbreak settings due to ethical and logistical constraints, provide the strongest evidence for causality when feasible.
The selection of one study design over another is influenced by several critical considerations. Ethical issues are often paramount, especially when exposure to a suspected harmful agent cannot be deliberately assigned. In such cases, observational designs are preferred to avoid harm while still generating meaningful evidence. Validity is another major consideration, encompassing both internal validity (the degree to which observed associations reflect true relationships) and external validity (the generalizability of findings to other populations). Efficiency, including time, cost, and feasibility, also plays a significant role, particularly in urgent outbreak scenarios where rapid evidence generation is required.
The choice of study design is shaped by the specific research questions being addressed. Some questions require estimation of disease frequency, while others focus on identifying risk factors or evaluating interventions. As a result, epidemiologists must carefully align their methodological approach with the scientific and public health objectives of the investigation. The process of conducting an epidemiological study is anchored in two fundamental steps: the formulation of a precise, testable hypothesis and the selection of an appropriate study design. These steps are interdependent and collectively determine the strength, relevance, and reliability of epidemiological evidence. A rigorous approach to both ensures that epidemiological investigations effectively contribute to understanding disease dynamics and informing public health action.
Epidemiological study designs and the determinants of disease distribution
1. Disease occurrence as a product of host-environment interaction and the need for systematic investigation
It is important to recognize that disease or infection does not arise in isolation or occur randomly within a population. Disease or infection emerges from a complex and dynamic interaction between a susceptible host (the individual), an infectious or causative agent, and a range of environmental and contextual factors that influence exposure, transmission, and susceptibility. This conceptual framework, often referred to as the epidemiological triad, underscores the fact that disease occurrence is inherently multifactorial. As such, understanding disease distribution requires more than simple observation; it demands a structured and systematic analytical approach capable of disentangling these interacting components.
The host component refers to the biological and behavioural characteristics of individuals that influence their susceptibility to disease. These include age, sex, genetic predisposition, immune status, nutritional status, comorbidities, and behavioural patterns such as hygiene practices or occupational exposures. The agent, on the other hand, may be biological (e.g., bacteria, viruses, parasites), chemical (e.g., toxins, pollutants), or physical (e.g., radiation). The environment encompasses all external factors that affect both the presence of the agent and the likelihood of host exposure, including physical conditions such as climate and sanitation, as well as social determinants such as population density, healthcare access, and socioeconomic status.
Because disease occurrence is the result of these interdependent factors, epidemiologists must adopt a logical and structured investigative approach when examining disease distribution within a community. Random or unsystematic observation is insufficient for identifying meaningful patterns or causal relationships. Instead, epidemiological inquiry relies on methodical data collection, careful classification of disease events, and analytical reasoning to identify associations between exposures and outcomes. This systematic approach allows researchers to move from simple descriptions of disease occurrence to deeper explanations of why diseases arise and how they spread within populations.
The interaction between host, agent, and environment is not static; it evolves over time and across different settings. For example, changes in environmental conditions such as rainfall, temperature, or sanitation infrastructure can alter the transmission dynamics of infectious diseases. Similarly, shifts in population behaviour, such as increased travel or changes in dietary habits, can influence exposure patterns. Epidemiological studies are therefore designed to capture these dynamic relationships through structured observation and analysis over time and space.
Epidemiology serves as a scientific bridge between observation and intervention. By systematically investigating how diseases are distributed and what factors contribute to their occurrence, epidemiologists can identify high-risk populations, detect emerging outbreaks, and generate evidence needed for public health action. This process is essential for transforming raw health data into actionable insights that inform disease prevention and control strategies.
2. Role of epidemiological study designs and considerations for their application
Epidemiological study designs play a crucial role in organizing and interpreting data in a structured manner that allows for the identification of disease agents, transmission patterns, and risk factors within a population. These designs provide a framework for classifying and analyzing health events, thereby enabling epidemiologists to distinguish between mere associations and potentially causal relationships. Through this structured approach, epidemiological studies not only describe disease occurrence but also support the development of targeted preventive and control measures aimed at reducing disease spread among unexposed or at-risk individuals.
One of the key strengths of epidemiological study designs is their ability to guide decision-making in public health practice. By systematically examining patterns of disease distribution, these studies help identify sources of infection, modes of transmission, and populations at increased risk. This information is essential for implementing appropriate interventions, such as vaccination programs, environmental sanitation measures, quarantine protocols, or health education campaigns. In outbreak situations, for instance, the rapid application of suitable study designs can help trace the origin of infection and prevent further transmission within the community.
The selection of an appropriate epidemiological study design is a critical decision that must be made carefully by researchers, epidemiologists, and public health practitioners. This decision is influenced by several interrelated factors that determine the feasibility, reliability, and overall success of the investigation. One of the primary considerations is cost, as different study designs vary significantly in terms of financial requirements. Large-scale cohort studies, for example, may require substantial funding due to long-term follow-up and extensive data collection, whereas case-control studies may be more cost-effective in certain outbreak scenarios.
Another important factor is practical feasibility, which includes considerations such as the availability of data, accessibility of the study population, and logistical constraints. In some settings, it may be difficult to track individuals over time or obtain accurate exposure histories, thereby limiting the suitability of certain study designs. The duration of the study is also a key consideration, particularly in situations where timely results are needed for urgent public health interventions. Cross-sectional or case-control designs may be preferred in such cases due to their relatively shorter time requirements compared to longitudinal cohort studies.
In addition to cost, feasibility, and duration, the expected type and quality of data also play a major role in determining the most appropriate study design. Researchers must consider whether the study aims to measure disease prevalence, incidence, or risk factors, as well as the level of precision required in the findings. The validity and reliability of the anticipated results are equally important, as different designs vary in their susceptibility to bias and confounding. Ethical considerations must also be taken into account, particularly when dealing with human populations and potential exposure to harmful agents.
The careful selection and application of epidemiological study designs ensure that disease investigations are both scientifically robust and practically relevant. By integrating methodological rigor with contextual considerations, epidemiologists are able to generate evidence that not only explains disease distribution but also informs effective prevention and control strategies. This systematic approach is essential for protecting population health and reducing the burden of disease within communities.
Classification of epidemiological studies: observational and experimental designs
Epidemiological studies are broadly categorized into observational and experimental designs, each serving distinct but interconnected roles in the investigation of disease and health outcomes. Observational studies provide essential insights into real-world disease patterns and risk factors, while experimental studies offer robust evidence for causal inference and intervention effectiveness. These two categories form the backbone of epidemiological research, enabling a comprehensive understanding of disease dynamics and supporting evidence-based public health action.
1. Observational epidemiological studies
Based on the fundamental principles of disease causation and distribution, epidemiological studies are broadly classified into two major categories: observational epidemiological studies and experimental epidemiological studies. This classification reflects the degree of investigator control over exposure conditions and the methodological purpose of the study. Observational studies form the largest and most commonly applied category in epidemiology, particularly in real-world public health settings where manipulation of exposures is either unethical or impractical.
Observational epidemiological studies are characterized by the fact that the researcher does not intervene or assign exposures to study participants. Instead, individuals are observed in their natural settings, and information is collected on exposures and outcomes as they occur organically within the population. This design is particularly useful for identifying associations between risk factors and disease outcomes, especially when experimental manipulation would be inappropriate or impossible. For example, it would be unethical to deliberately expose individuals to a suspected carcinogen or infectious agent; therefore, observational approaches are required to study such relationships.
Observational studies are typically further subdivided into descriptive and analytical designs. Descriptive observational studies focus on characterizing the distribution of disease by person, place, and time. They provide essential baseline data on disease frequency and patterns within populations and are often the first step in outbreak investigations. These studies help generate hypotheses by identifying unusual trends or clusters of disease that warrant further investigation. Common measures used in descriptive epidemiology include incidence, prevalence, and mortality rates, which collectively provide a quantitative understanding of disease burden.
Analytical observational studies are designed to test specific hypotheses about the relationship between exposures and outcomes. These include cohort studies, case-control studies, and cross-sectional studies. Cohort studies follow groups of individuals over time based on their exposure status to determine the incidence of disease, allowing for the establishment of temporal relationships between exposure and outcome. Case-control studies begin with individuals who already have the disease (cases) and compare them to individuals without the disease (controls) to retrospectively assess exposure history. Cross-sectional studies assess exposure and outcome simultaneously within a population, providing a snapshot of disease prevalence and associated factors at a single point in time.
Each of these observational designs has distinct advantages and limitations. Cohort studies are particularly strong in establishing temporal relationships and calculating incidence rates but can be time-consuming and expensive. Case-control studies are efficient for studying rare diseases or diseases with long latency periods but are more susceptible to recall and selection bias. Cross-sectional studies are relatively quick and inexpensive but are limited in their ability to infer causality due to the simultaneous measurement of exposure and outcome.
Despite these limitations, observational epidemiological studies are indispensable in public health research. They provide critical insights into real-world disease dynamics, especially in complex systems where multiple interacting risk factors are present. They are also essential for studying chronic diseases, environmental exposures, occupational hazards, and emerging infectious diseases. In many cases, observational evidence forms the foundation for policy decisions and guides the development of preventive interventions before experimental confirmation is possible.
Observational studies play a key role in identifying vulnerable populations and health disparities. By examining how disease occurrence varies across demographic, geographic, and socioeconomic groups, epidemiologists can uncover structural and behavioural determinants of health outcomes. This information is vital for designing targeted interventions and allocating healthcare resources efficiently.
2. Experimental epidemiological studies
In contrast to observational approaches, experimental epidemiological studies are characterized by active intervention by the investigator. In this category of study design, the researcher deliberately assigns exposures or interventions to study participants and observes the resulting effects on health outcomes. This controlled manipulation of exposure distinguishes experimental studies from observational ones and provides a stronger basis for establishing causal relationships.
Experimental epidemiological studies are often considered the gold standard for evaluating the effectiveness of interventions due to their ability to minimize bias and confounding. The most well-known form of experimental study is the randomized controlled trial (RCT), in which participants are randomly assigned to either an intervention group or a control group. Randomization ensures that known and unknown confounding variables are evenly distributed between groups, thereby increasing the internal validity of the study.
In public health and clinical research, experimental studies are commonly used to evaluate vaccines, pharmaceuticals, behavioural interventions, and preventive strategies. For example, vaccine trials assess whether immunization reduces the incidence of infectious disease compared to a placebo or standard care group. Similarly, clinical trials may evaluate the effectiveness of new drugs in treating chronic conditions such as hypertension, diabetes, or infectious diseases.
Experimental studies are typically structured in phases, particularly in pharmaceutical research. Early-phase trials (Phase I and II) focus on safety, dosage, and preliminary efficacy, while later-phase trials (Phase III and IV)evaluate effectiveness in larger populations and monitor long-term outcomes. This phased approach ensures that interventions are rigorously tested before widespread implementation.
One of the major strengths of experimental epidemiological studies is their high level of internal validity. Because the investigator controls the exposure and uses randomization, the likelihood of confounding and selection bias is significantly reduced. This allows for a more confident interpretation of causal relationships between exposure and outcome. Additionally, blinding techniques, such as single-blind or double-blind designs, are often employed to further reduce bias by preventing participants and researchers from knowing group assignments.
Experimental studies also have important limitations. Ethical considerations are a major constraint, as it is often impossible or unethical to deliberately expose individuals to harmful agents or risky conditions. For example, researchers cannot ethically assign individuals to smoke cigarettes or be exposed to known carcinogens. As a result, experimental designs are largely restricted to interventions that are considered safe or potentially beneficial.
Another limitation is cost and complexity. Experimental studies, particularly large-scale randomized controlled trials, require substantial financial resources, extensive infrastructure, and long follow-up periods. They also demand strict regulatory oversight and careful monitoring to ensure participant safety and data integrity. In addition, experimental studies may have limited external validity, meaning that their findings may not always be generalizable to broader populations due to strict inclusion and exclusion criteria.
Despite these challenges, experimental epidemiological studies remain essential for advancing medical and public health knowledge. They provide the most reliable evidence for determining whether an intervention truly causes a change in health outcomes. In many cases, experimental findings are used to confirm or refine hypotheses generated from observational studies, creating a complementary relationship between the two approaches.
References
Aschengrau A and Seage G.R (2013). Essentials of Epidemiology in Public Health. Third edition. Jones and Bartleh Learning,
Aschengrau, A., & G. R. Seage III. (2009). Essentials of Epidemiology in Public Health. Boston: Jones and Bartlett Publishers.
Bonita R., Beaglehole R., Kjellström T (2006). Basic epidemiology. 2nd edition. World Health Organization. Pp. 1-226.
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA.
Castillo-Salgado C (2010). Trends and directions of global public health surveillance. Epidemiol Rev, 32:93–109.
Centers for Disease Control and National Institutes of Health (1999). Biosafety in Microbiological and Biomedical Laboratories, 4th edn, Washington DC: CDC.
Gordis L (2013). Epidemiology. Fifth edition. Saunders Publishers, USA.
Guillemin J (2006). Scientists and the history of biological weapons. European Molecular Biology Organization (EMBO) Reports, Vol 7, Special Issue: S45-S49.
Halliday JE, Meredith AL, Knobel DL, Shaw DJ, Bronsvoort BMC, Cleaveland S (2007). A framework for evaluating animals as sentinels for infectious disease surveillance. J R Soc Interface, 4:973–984.
Lucas A.O and Gilles H.M (2003). Short Textbook of Public Health Medicine for the tropics. Fourth edition. Hodder Arnold Publication, UK.
MacMahon B., Trichopoulos D (1996). Epidemiology Principles and Methods. 2nd ed. Boston, MA: Little, Brown and Company. USA.
Nelson K.E and Williams C (2013). Infectious Disease Epidemiology: Theory and Practice. Third edition. Jones and Bartleh Learning.
Porta M (2008). A dictionary of epidemiology. 5th edition. New York: Oxford University Press.
Rothman K.J and Greenland S (1998). Modern epidemiology, 2nd edition. Philadelphia: Lippincott-Raven.
Rothman K.J, Greenland S and Lash T.L (2011). Modern Epidemiology. Third edition. Lippincott Williams and Wilkins, Philadelphia, PA, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.