Descriptive epidemiology is a foundational branch of epidemiology concerned with characterizing the distribution of health-related events within populations. It focuses on answering three core questions: who is affected, where cases occur, and when events take place. By systematically organizing health data according to person, place, and time, descriptive epidemiology provides the essential first step in understanding disease patterns and generating hypotheses for further investigation. It does not primarily aim to test causal relationships but instead establishes the basic epidemiological profile of diseases or health conditions within defined populations.
Descriptive epidemiology is a fundamental component of public health that focuses on characterizing disease distribution by person, place, and time. It serves critical functions in surveillance, outbreak detection, health planning, and hypothesis generation. While it does not establish causality, it provides the essential descriptive foundation upon which analytical epidemiology builds. Understanding its definition, purpose, and role in public health is essential for interpreting disease patterns and guiding effective interventions.
Descriptive epidemiology can be defined as the study of the frequency and distribution of diseases or health outcomes in populations according to person, place, and time variables. It is primarily concerned with describing the occurrence of disease rather than explaining why it occurs. In practice, it involves the collection, organization, and presentation of health data in a manner that highlights patterns and trends.
The primary purpose of descriptive epidemiology is to generate a clear and structured picture of disease burden within a population. This includes identifying which groups are most affected, the geographical areas with higher disease occurrence, and the time periods during which cases are more frequent. Such information is crucial for identifying at-risk populations and guiding public health interventions.
Another important purpose is hypothesis generation. By identifying unusual patterns or clusters of disease, descriptive studies help epidemiologists formulate hypotheses about potential risk factors or causes. For example, a sudden increase in respiratory illness in a specific region may prompt further analytical studies to investigate environmental exposures or infectious agents.
Descriptive epidemiology serves as a tool for health planning and resource allocation. Health authorities rely on descriptive data to determine where to allocate medical resources, design prevention strategies, and evaluate the burden of disease across different population groups.
Role of descriptive epidemiological studies in public health and disease surveillance
Descriptive epidemiology plays a central role in public health practice and disease surveillance systems. Surveillance systems continuously collect, analyze, and interpret health data to monitor the occurrence and spread of diseases. Descriptive epidemiology provides the framework for organizing this data in a meaningful way. In disease surveillance, descriptive epidemiology enables public health professionals to detect outbreaks early, monitor trends over time, and assess the effectiveness of interventions. For example, tracking the number of influenza cases over multiple seasons allows health authorities to anticipate peak periods and prepare healthcare systems accordingly. Similarly, monitoring vaccination coverage across regions helps identify gaps in immunization programs.
Descriptive epidemiology is also essential during outbreak investigations. When a new disease cluster is identified, the first step is to describe the affected population in terms of who is getting sick, where the cases are located, and when symptoms began. This initial descriptive analysis often provides critical clues about the source and mode of transmission of the disease. Beyond infectious diseases, descriptive epidemiology is widely used in the study of chronic diseases such as diabetes, cancer, and cardiovascular conditions. It helps identify trends in disease prevalence, demographic disparities, and geographical variations, all of which are important for long-term public health planning.
Descriptive epidemiology supports evidence-based policy making. Governments and health organizations use descriptive data to prioritize health issues, design intervention programs, and evaluate progress toward public health goals. Without accurate descriptive data, it would be difficult to understand the scale and distribution of health problems within populations.
Differences between descriptive and analytical epidemiological studies
Although descriptive and analytical epidemiology are closely related, they differ significantly in purpose, design, and outcomes. Descriptive epidemiology is primarily concerned with describing the distribution of disease. It focuses on answering “what is happening?” rather than “why it is happening?” It relies on observational data and often uses simple statistical measures such as incidence, prevalence, and mortality rates. Common study designs include cross-sectional studies, case reports, and ecological studies. On the other hand, analytical epidemiology is designed to test hypotheses and determine causal relationships between exposures and outcomes. It seeks to answer questions such as “why is this disease occurring?” or “what factors increase the risk of disease?” Analytical studies typically include cohort studies, case-control studies, and randomized controlled trials. These designs allow for comparison between exposed and unexposed groups to assess associations and infer causality.
Another key difference lies in the level of complexity and inference. Descriptive epidemiology provides the foundational data needed to generate hypotheses, whereas analytical epidemiology builds upon this foundation to test and refine those hypotheses using more rigorous statistical methods. Descriptive studies are generally faster, less expensive, and easier to conduct, making them particularly useful in the early stages of public health investigations. Analytical studies, on the other hand, require more detailed data collection, careful control of confounding variables, and more advanced statistical analysis. Despite these differences, both approaches are complementary. Descriptive epidemiology lays the groundwork by identifying patterns and trends, while analytical epidemiology explains the underlying causes of those patterns. Together, they form a continuous process in epidemiological research that advances understanding of disease dynamics and informs effective public health action.
Measures used in descriptive epidemiological studies
Descriptive epidemiology relies on a set of quantitative measures that summarize the frequency and distribution of health-related events in populations. These measures are fundamental for characterizing disease burden, identifying high-risk groups, monitoring trends over time, and informing public health planning. Among the most important are incidence and prevalence, mortality and morbidity rates, and attack rate and case fatality rate. Each measure provides a distinct perspective on disease occurrence and severity.
The core measures in descriptive epidemiological studies are:
- Incidence and prevalence,
- Mortality and morbidity rates,
- Attack rate and
- Case fatality rate are
These core measures provide complementary insights into disease frequency, distribution, and severity. These measures are essential for surveillance, outbreak investigation, resource allocation, and evaluating the effectiveness of public health interventions.
- Incidence and Prevalence
Incidence refers to the occurrence of new cases of a disease or health condition within a defined population over a specified period of time. It is a measure of risk and is particularly useful for studying disease causation and evaluating preventive interventions. Incidence can be expressed in two main forms:
- Cumulative incidence (incidence proportion): the proportion of a population that develops a disease over a given period.
- Incidence rate (incidence density): the number of new cases per unit of person-time (e.g., person-years).
Incidence is especially valuable in acute diseases or conditions where the onset of disease can be clearly identified, such as infectious disease outbreaks or newly diagnosed cancers.
On the other hand, prevalence measures the total number of existing cases (both new and pre-existing) of a disease in a population at a specific point in time or over a period. It reflects the overall burden of disease in a population rather than risk. Prevalence is commonly divided into:
- Point prevalence: This is the proportion of individuals with the disease at a specific point in time.
- Period prevalence: This is the proportion of individuals who have had the disease at any time during a specified period.
Prevalence is influenced by both incidence and disease duration. Diseases with long duration and low mortality (e.g., diabetes) tend to have high prevalence, whereas diseases with short duration or high fatality (e.g., some acute infections) may have low prevalence even if incidence is high.
- Mortality and Morbidity Rates
Mortality rates measure the frequency of deaths in a population over a specific time period. They are key indicators of population health and healthcare effectiveness. Common forms include:
- Crude mortality rate: This is the total deaths in a population per unit time.
- Cause-specific mortality rate: This is the deaths attributed to a specific disease.
- Age-specific mortality rate: This is the deaths within a defined age group.
- Infant mortality rate: This is the deaths of infants under one year per 1,000 live births.
Mortality rates help identify leading causes of death and assess the impact of public health interventions, such as vaccination programs or improved healthcare access. Morbidity rates, on the other hand, describe the occurrence of disease or illness in a population. Unlike mortality, morbidity captures non-fatal health outcomes and provides insight into disease burden beyond death. Morbidity measures include incidence and prevalence, but also specific indicators such as hospital admission rates, disability rates, and outpatient visit rates. Morbidity data are essential for understanding the impact of chronic diseases and non-fatal conditions on quality of life and healthcare systems. Both mortality and morbidity rates provide a comprehensive picture of population health by capturing both fatal and non-fatal outcomes.
Attack Rate and Case Fatality Rate
The attack rate is a specialized incidence measure commonly used in outbreak investigations. It represents the proportion of an at-risk population that develops disease during a specific, often short, time period. It is typically used in settings where exposure is well defined, such as foodborne illness outbreaks or infectious disease clusters. The attack rate helps identify the source of infection and assess the speed and extent of disease spread. It is calculated as:
Attack rate = (Number of new cases during outbreak / Population at risk during outbreak) × 100
There are also secondary attack rates, which measure transmission among close contacts of primary cases, such as household members. This is particularly useful for understanding person-to-person spread. The case fatality rate (CFR) measures the severity of a disease by estimating the proportion of diagnosed cases that result in death over a specified period. It is a key indicator in assessing the lethality of diseases and guiding clinical and public health responses. CFR is calculated as:
CFR = (Number of deaths from a disease / Number of diagnosed cases of that disease) × 100
A high CFR indicates a more severe disease or limited access to effective treatment, while a low CFR may reflect better healthcare management or a less virulent disease strain. However, CFR can be influenced by case detection bias, especially if mild cases are underreported.
Descriptive epidemiological variables: person, place, and time
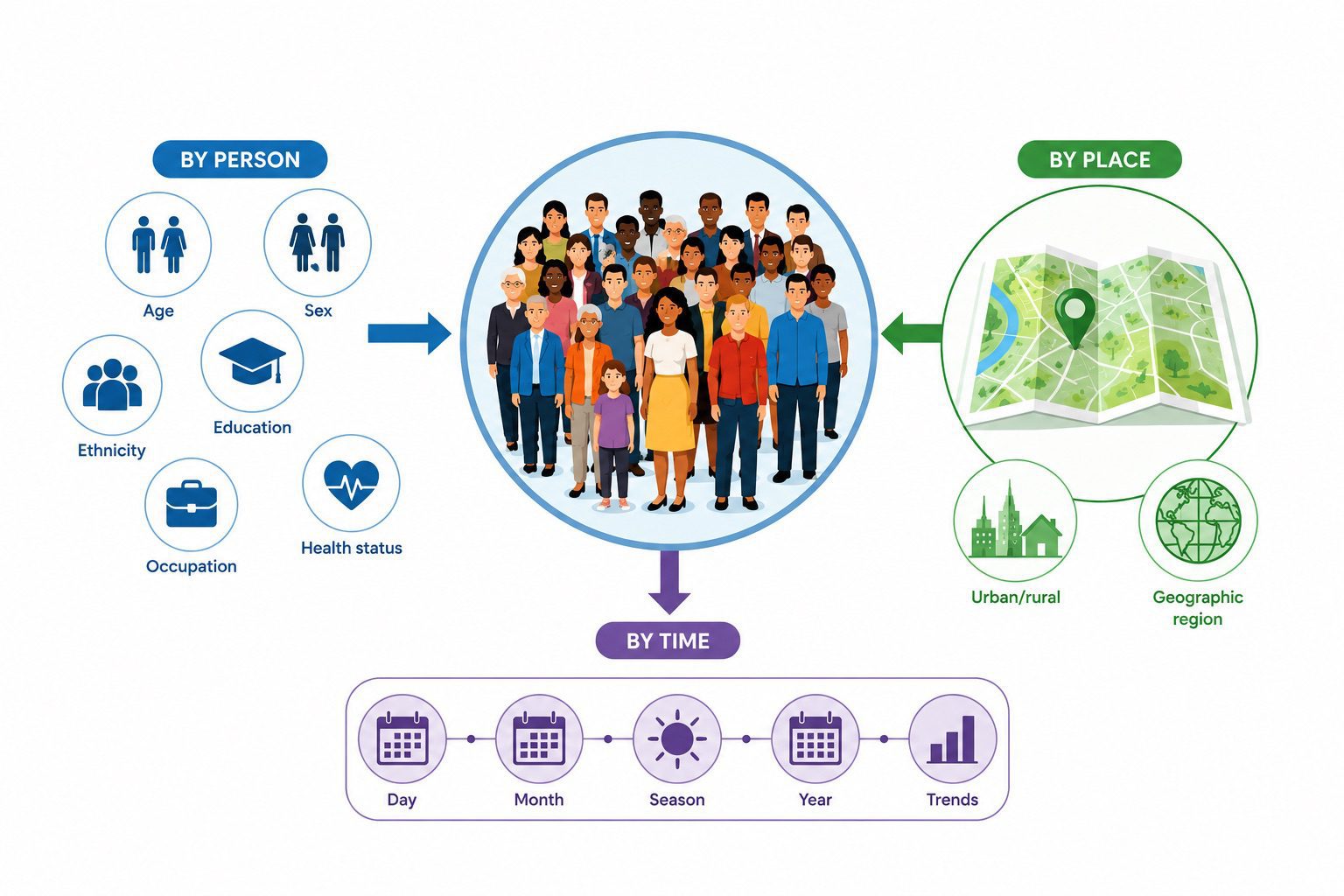
Descriptive epidemiology is fundamentally concerned with characterizing the distribution of health-related events within populations. Its core analytical framework is built on three interdependent variables: person, place, and time. These variables are essential for organizing surveillance data, generating hypotheses, identifying at-risk populations, and guiding public health interventions. Together, they provide a structured way to understand who is affected, where the disease occurs, and when it happens.
The triad of person, place, and time forms the backbone of descriptive epidemiology (Figure 1). Each variable provides a distinct yet interconnected perspective on disease distribution. Person variables identify who is at risk, place variables reveal where risks are concentrated, and time variables explain when disease patterns occur. This triad enable public health professionals to generate hypotheses, detect outbreaks, and design targeted interventions. A thorough understanding of these variables is essential for effective disease surveillance and evidence-based public health practice.

1. Person characteristics in descriptive epidemiological study
The person component focuses on the demographic, biological, behavioral, and social attributes that influence disease distribution. It answers the question: Who is affected? One of the most fundamental person variables is age. Many diseases show strong age-specific patterns due to biological susceptibility and cumulative exposure. For example, infectious diseases such as measles often disproportionately affect children, while chronic conditions like cardiovascular disease and cancer are more prevalent in older populations. Age-specific rates are therefore critical for identifying vulnerable groups and planning targeted interventions such as immunization schedules or screening programs.
Sex (or gender) is another key determinant. Differences in disease prevalence between males and females may arise from biological factors (e.g., hormonal influences, genetic susceptibility) or sociocultural determinants (e.g., occupational exposure, health-seeking behavior). For instance, men may exhibit higher rates of occupational injuries in physically demanding industries, while women may show higher rates of autoimmune conditions. Occupation plays a significant role in shaping exposure risk. Certain professions are associated with specific hazards; healthcare workers may be exposed to infectious agents, miners to dust-related lung diseases, and agricultural workers to pesticide exposure. Occupational epidemiology often overlaps with descriptive epidemiology by identifying patterns of disease among workforce groups and informing workplace safety regulations.
Ethnicity and socioeconomic status (SES) also contribute significantly to disease distribution. Ethnic disparities may reflect genetic predispositions, but more often they indicate structural inequalities such as access to healthcare, environmental exposures, and discrimination. Similarly, low SES is strongly associated with increased risk of infectious diseases, malnutrition, and chronic illnesses due to limited access to preventive care and healthy living conditions. Additional person variables include behavioral factors such as smoking, diet, physical activity, and substance use. These behaviors are often clustered within populations and strongly influence non-communicable disease patterns. Understanding these attributes helps epidemiologists identify high-risk subgroups and tailor health promotion strategies.
2. Place Distribution in Descriptive Epidemiology
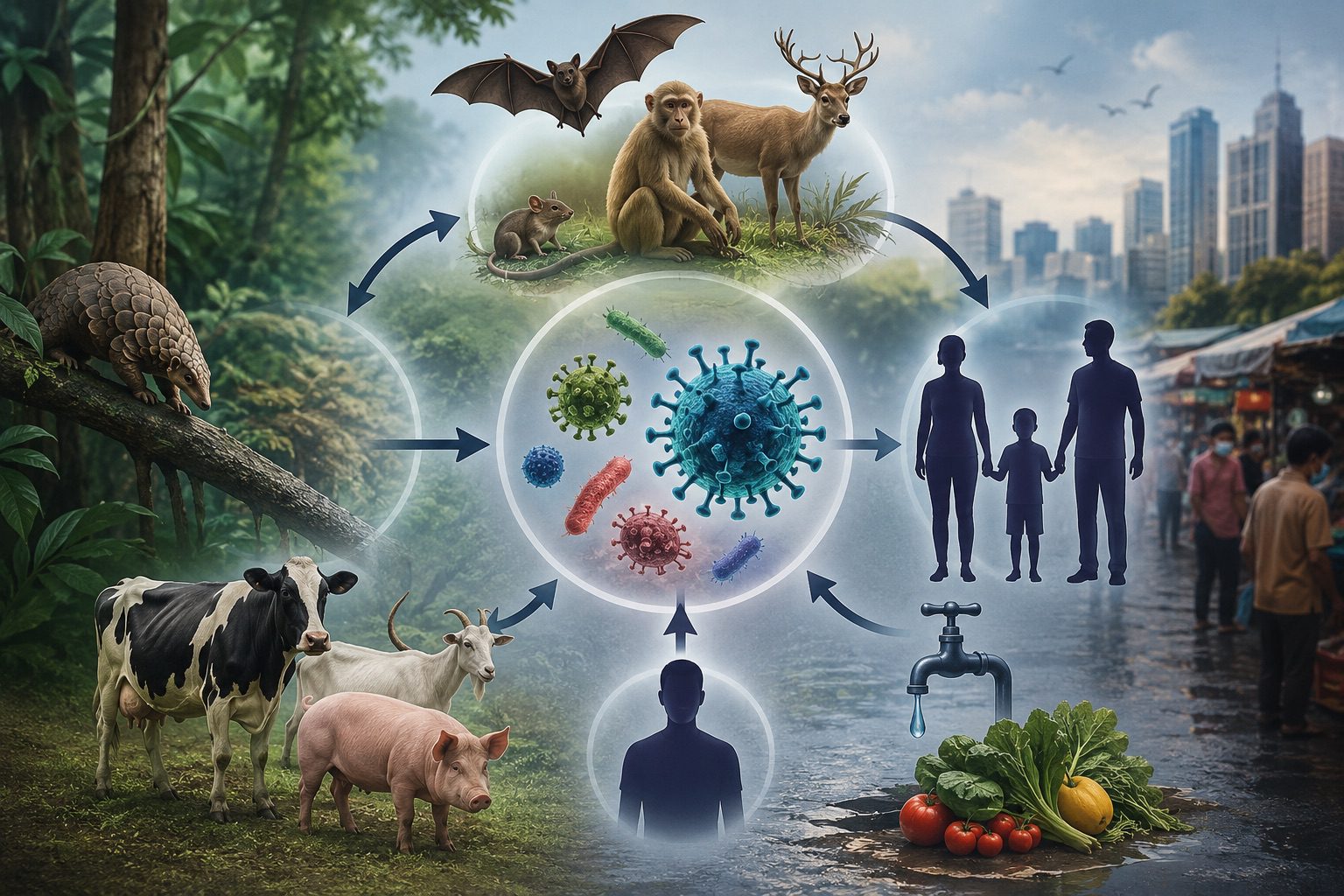
The place variable describes the geographical distribution of disease occurrence. It addresses the question: Where is the disease occurring? Place can be analyzed at multiple spatial levels, including global, national, regional, community, or even household levels. Geographic mapping of disease incidence helps identify clusters, hotspots, or areas of unusually high or low risk. These spatial patterns may indicate environmental exposures, cultural practices, or healthcare access differences. A common distinction in place analysis is between urban and rural settings. Urban areas may show higher rates of respiratory diseases due to pollution, while rural areas may experience higher burdens of zoonotic infections or limited access to healthcare services. Migration between these settings can also alter disease dynamics, particularly for infectious diseases.
Environmental factors such as climate, altitude, water quality, and sanitation infrastructure are central to place-based epidemiology. For example, malaria is more prevalent in tropical and subtropical regions due to favorable mosquito breeding conditions. Similarly, waterborne diseases tend to cluster in regions with poor sanitation systems. Spatial epidemiology often uses geographic information systems (GIS) to visualize and analyze disease distribution. These tools allow for precise identification of clusters and facilitate resource allocation. Place-based analysis is particularly important in outbreak investigations, where identifying a common geographic source can help trace the origin of infection.
3. Time Trends in Descriptive Epidemiology
The time variable examines how disease occurrence changes over time. It answers the question: When is the disease occurring? Time trends are typically categorized into short-term, seasonal, cyclic, and long-term (secular) trends. Each provides different epidemiological insights. Short-term fluctuations often relate to outbreaks or epidemics, where disease incidence increases sharply over a brief period. For example, foodborne illness outbreaks may occur suddenly due to contaminated food sources. Seasonal trends refer to predictable changes in disease frequency at certain times of the year. Influenza, for instance, peaks during colder months in temperate regions, while vector-borne diseases like dengue often increase during rainy seasons when mosquito populations expand.
Cyclic trends involve periodic fluctuations occurring over longer intervals, often influenced by changes in herd immunity, pathogen evolution, or population dynamics. Some infectious diseases exhibit multi-year cycles due to variations in susceptibility and exposure. Secular trends describe long-term changes in disease patterns over decades. These trends may reflect improvements in healthcare, vaccination programs, changes in lifestyle, or environmental modifications. For example, the global decline in measles incidence over the past several decades reflects widespread immunization efforts. Time analysis is essential for identifying emerging health threats, evaluating intervention effectiveness, and forecasting future disease burdens. Epidemiologists often use time-series analysis to detect deviations from expected patterns.
Study designs in descriptive epidemiological studies
Descriptive epidemiology is concerned with characterizing the distribution of health-related events in populations according to person, place, and time. Its primary objective is not to test hypotheses about causation but to generate them by systematically describing disease patterns. Within this framework, several key study designs are used: case reports and case series, cross-sectional studies, ecological studies, and disease surveillance systems. Each design has distinct methodological features, strengths, and limitations, and each contributes uniquely to public health understanding and decision-making.
Case reports and case series
Case reports and case series provide early signals of new or rare conditions. A case report is a detailed description of a single patient with an unusual or novel disease presentation, treatment response, or clinical outcome. It typically includes clinical history, diagnostic findings, therapeutic interventions, and follow-up results. Case reports are especially valuable in identifying new diseases, rare conditions, or unexpected adverse effects of medical interventions. For example, early reports of AIDS in the 1980s were initially documented as case reports describing unusual opportunistic infections in otherwise healthy individuals.
A case series extends this concept by describing multiple patients with similar conditions. Unlike case reports, case series can identify patterns across individuals, such as common symptoms, exposures, or clinical outcomes. However, they still lack a comparison (control) group, which limits their ability to establish causality or measure risk.
Despite these limitations, case reports and case series play a crucial role in signal detection in medicine and epidemiology. They are often the first step in identifying emerging health threats, rare diseases, or novel side effects of drugs and vaccines. Their major strengths include simplicity, low cost, and the ability to generate early hypotheses. However, they are highly susceptible to selection bias and cannot provide incidence or prevalence estimates.
Cross-sectional studies
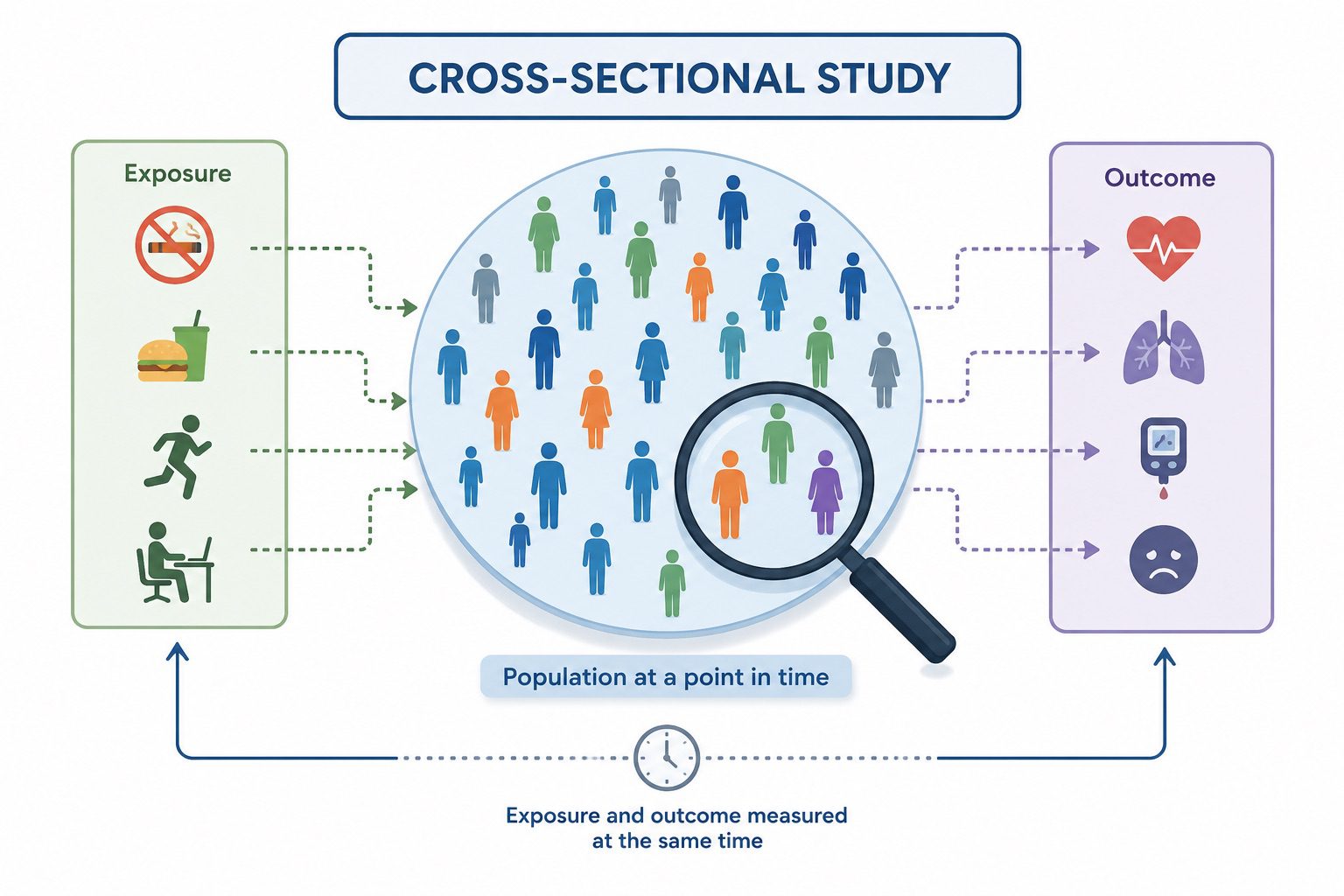
Cross-sectional studies examine the distribution of diseases or health-related characteristics in a population at a single point in time. They provide a “snapshot” of the population, simultaneously measuring exposure and outcome status. This design is widely used in public health surveys, such as national health and nutrition examinations, mental health prevalence studies, and risk factor assessments. Cross-sectional studies quantify disease burden and identify potential associations.
A key measure derived from cross-sectional studies is prevalence, which reflects the proportion of individuals in a population who have a disease at a specific time. This makes cross-sectional studies particularly useful for assessing the burden of chronic diseases such as diabetes, hypertension, or obesity. One of the strengths of cross-sectional studies is their efficiency. They are relatively quick, cost-effective, and useful for generating hypotheses about associations between exposures and outcomes. They are also valuable for planning healthcare services because they provide data on the current health status of a population.
However, a major limitation is the inability to establish temporal relationships between exposure and disease. Since exposure and outcome are measured simultaneously, it is often unclear whether the exposure preceded the disease or vice versa. This restricts causal inference and makes cross-sectional studies more suitable for hypothesis generation rather than hypothesis testing.
Ecological studies
Ecological studies analyze data at the group or population level rather than at the individual level. Units of analysis may include countries, regions, cities, schools, or workplaces. For example, researchers might compare lung cancer rates across countries with different levels of smoking prevalence or examine the relationship between air pollution levels and respiratory disease rates across cities. Ecological studies explore population-level patterns and generate broad hypotheses. The defining feature of ecological studies is that both exposure and outcome data are aggregated. This allows researchers to explore broad patterns and generate hypotheses about environmental, social, or policy-related determinants of health.
Ecological studies are particularly useful when individual-level data are unavailable or when studying large-scale exposures such as environmental pollution, socioeconomic conditions, or national health policies. They are also relatively inexpensive and can utilize existing datasets. However, ecological studies are vulnerable to the ecological fallacy, which occurs when associations observed at the group level are incorrectly assumed to apply to individuals. For example, even if countries with higher fat consumption have higher rates of heart disease, it does not necessarily mean that individuals who consume more fat are at higher risk within those countries. This limitation makes ecological studies less suitable for causal inference at the individual level.
Disease surveillance systems
Disease surveillance systems are systematic and continuous processes of data collection, analysis, interpretation, and dissemination of health information. Disease surveillance systems ensure continuous monitoring and early detection of health threats. Unlike other descriptive study designs, surveillance is an ongoing public health function rather than a one-time study. Its primary goal is to monitor disease trends, detect outbreaks early, and inform public health interventions. Surveillance systems can be passive, active, or sentinel. In passive surveillance, healthcare providers routinely report cases of diseases to health authorities. In active surveillance, public health officials actively seek out cases, often during outbreaks.
Sentinel surveillance involves selected reporting sites that provide high-quality data on specific diseases. Examples of such diseases include influenza surveillance networks, HIV reporting systems, and notifiable disease registries. These systems are essential for detecting emerging infectious diseases, monitoring vaccination coverage, and evaluating the effectiveness of public health programs. The strengths of surveillance systems lie in their ability to provide continuous, real-time data for decision-making. They are fundamental to outbreak detection and control. However, their effectiveness depends on data quality, reporting compliance, and system coverage. Underreporting, delays, and inconsistencies can reduce their accuracy and usefulness.
Applications, Strengths, and Limitations of Descriptive Epidemiological Studies
Descriptive epidemiological studies are a foundational component of public health practice, primarily used to characterize the distribution of disease and other health-related events within populations. By systematically organizing data according to person, place, and time, they provide essential insights that support disease surveillance, outbreak detection, and health system planning. In this capacity, descriptive studies are indispensable for identifying patterns of health events and generating hypotheses that guide further investigation within the broader epidemiological framework.
Their key strengths include simplicity, cost-effectiveness, and rapid applicability, making them well-suited for routine surveillance and urgent public health responses. They are particularly valuable in summarizing population-level trends and informing policy and resource allocation. However, despite these advantages, descriptive epidemiology is inherently limited in its ability to establish causal relationships. It is also vulnerable to data quality issues, such as underreporting, misclassification, and incomplete datasets, which can affect interpretation. While descriptive studies provide the essential first step in understanding population health problems, they must be complemented by analytical epidemiological designs to test hypotheses and assess causality.
Applications of descriptive epidemiological studies
1. Disease outbreak investigations
One of the most immediate and practical applications of descriptive epidemiology is in the investigation of disease outbreaks. When an unusual increase in disease incidence is detected, descriptive methods are used first to define the outbreak in terms of who is affected, where cases are occurring, and when they are occurring. This triad: person, place, and time helps epidemiologists construct an initial profile of the outbreak. For example, analyzing age distribution may reveal that a particular age group is disproportionately affected, suggesting potential exposure patterns or vulnerabilities. Geographic clustering can identify potential environmental or institutional sources, such as contaminated water supplies or healthcare-associated transmission. Temporal trends, such as epidemic curves, help determine whether an outbreak is point-source, continuous, or propagated. This early-stage analysis is crucial for guiding immediate public health interventions, such as isolation measures, vaccination campaigns, or environmental remediation. It also provides the basis for generating hypotheses that are later tested using analytical epidemiological designs.
2. Health planning and policy development
Descriptive epidemiology plays a central role in informing health planning and policy formulation. By quantifying disease burden and identifying patterns of distribution across populations, it enables policymakers to allocate resources efficiently and equitably. For instance, prevalence data can highlight chronic disease burdens in specific populations, guiding the establishment of specialized clinics or prevention programs. Mortality statistics may reveal leading causes of death within a region, prompting targeted interventions such as cardiovascular disease prevention initiatives or maternal health programs. Additionally, time trend analyses can identify emerging health threats, such as increasing rates of diabetes or antimicrobial resistance, allowing for proactive policy responses. At the population level, descriptive epidemiological data support needs assessments, prioritization of health services, and evaluation of public health interventions. Without such baseline information, health systems would lack the empirical foundation required for rational planning and resource distribution.
3. Surveillance and monitoring of disease trends
Another key application of descriptive epidemiology is in public health surveillance systems. Continuous collection, analysis, and interpretation of health data enable the detection of changes in disease patterns over time. Surveillance data are essential for early warning systems, particularly for infectious diseases with epidemic potential. For example, monitoring influenza-like illness rates allows health authorities to anticipate seasonal outbreaks and prepare healthcare systems accordingly. Similarly, tracking non-communicable diseases provides insight into long-term epidemiological transitions within populations. Descriptive surveillance also supports evaluation of interventions by comparing disease trends before and after implementation of public health programs, although causal inference remains limited.
Strengths of descriptive epidemiological studies
One of the primary strengths of descriptive epidemiology is its simplicity and accessibility. These studies often rely on routinely collected data, such as hospital records, death certificates, or surveillance databases, making them relatively inexpensive and feasible even in resource-limited settings. They can be conducted quickly, which is particularly valuable during emerging public health threats. Another strength lies in their ability to generate hypotheses. By identifying unusual patterns or clusters of disease, descriptive studies provide the foundation for more rigorous analytical investigations. For example, an observed increase in gastrointestinal illness in a specific geographic area may lead to case-control or cohort studies to identify the source of contamination.
Descriptive epidemiology is also essential for understanding disease burden. It provides fundamental measures such as incidence, prevalence, and mortality rates, which are critical for comparing health outcomes across populations and over time. These measures allow for identification of high-risk groups and inform targeted interventions. Additionally, these studies enhance communication in public health. The clear presentation of data through maps, epidemic curves, and demographic tables makes complex health information more understandable to policymakers, stakeholders, and the general public.
Limitations of descriptive epidemiological studies
Despite their utility, descriptive epidemiological studies have important limitations, particularly in relation to causal inference. The most significant limitation is their inability to establish cause-and-effect relationships. While they can identify associations or patterns, they do not control for confounding variables or bias, making it impossible to determine whether observed relationships are causal or coincidental. Another limitation is the potential for data quality issues. Descriptive studies often rely on secondary data sources, which may suffer from underreporting, misclassification, or incomplete records. These issues can distort true disease patterns and lead to inaccurate conclusions.
Descriptive studies are limited in analytical depth. They do not test specific hypotheses or quantify the strength of associations between exposures and outcomes. As a result, they must be complemented by analytical epidemiological designs, such as cohort or case-control studies, to explore causal mechanisms. There is also a risk of ecological fallacy, particularly in ecological studies, where inferences about individuals are made based on group-level data. This can lead to incorrect assumptions about risk factors at the individual level. Descriptive epidemiology may be influenced by surveillance bias. Populations with better access to healthcare or more robust reporting systems may appear to have higher disease rates simply because of more complete data collection, rather than true differences in disease occurrence.
References
Aschengrau A and Seage G.R (2013). Essentials of Epidemiology in Public Health. Third edition. Jones and Bartleh Learning,
Aschengrau, A., & G. R. Seage III. (2009). Essentials of Epidemiology in Public Health. Boston: Jones and Bartlett Publishers.
Bonita R., Beaglehole R., Kjellström T (2006). Basic epidemiology. 2nd edition. World Health Organization. Pp. 1-226.
Lucas A.O and Gilles H.M (2003). Short Textbook of Public Health Medicine for the tropics. Fourth edition. Hodder Arnold Publication, UK.
MacMahon B., Trichopoulos D (1996). Epidemiology Principles and Methods. 2nd ed. Boston, MA: Little, Brown and Company. USA.
Nelson K.E and Williams C (2013). Infectious Disease Epidemiology: Theory and Practice. Third edition. Jones and Bartleh Learning.
Porta M (2008). A dictionary of epidemiology. 5th edition. New York: Oxford University Press.
Rothman K.J and Greenland S (1998). Modern epidemiology, 2nd edition. Philadelphia: Lippincott-Raven.
Rothman K.J, Greenland S and Lash T.L (2011). Modern Epidemiology. Third edition. Lippincott Williams and Wilkins, Philadelphia, PA, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.