Vibrio cholerae is a Gram-negative, oxidase positive, spiral, non-spore forming, facultative, motile, curved or straight rod bacterium that causes severe diarrheal disease known as cholera in humans. Cholera, which is one of the leading causes of waterborne infections in developing countries, is a profuse watery diarrheal disease that is associated with extreme dehydration following excessive water loss from the body that can lead to death if not controlled. V. cholerae is of the family Vibronaceae, and it is commonly found on the surface of waters across the world. Out of all the species of Vibrio, only V. cholerae and V. parahaemolyticus that are the most important pathogens of humans, and these and other species of Vibrio are found in both saltwater and freshwater and in association with other aquatic life including Phytoplanktons and shellfish.
Though several O antigen (i.e. somatic or cell wall antigen) serotypes of V. cholerae exists, only serotypes O1 and O139 are known to cause severe diarrheal disease (cholera) in humans. The O1 serotypes are further divided into two serotypes (Ogawa and Inaba) and two biotypes (E1 Tor and Classical). These serotypes and biotypes of V. cholerae have been implicated in most of the cholera epidemics that occurred in parts of Africa, Asia and the Americas (South and Central). Cholera is an endemic water-borne disease in about 100 countries, and the disease is mostly common in developing countries including Africa, Asia and some parts of Central and South America. In 2013 (September and October in particular), cholera outbreak occurred in seven (7) Nigerian states resulting in 2771 cases and 124 deaths with a case fatality rate (CFR) of 4.5%.
This outbreak was largely attributed to poor sanitation, lack of access to drinking water and lack of good toilet facilities. Cholera is still an endemic bacterial infection in most parts of the sub-Saharan Africa, and its cause and spread is largely attributed to poor personal hygiene and feacal contamination of drinking water sources. V. cholerae serotypes O1 and O139 are largely responsible for the world’s cholera epidemic and pandemic, and these cause secretary non-inflammatory diarrheal disease in places where it occurs. Cholera is not an invasive infection, thus it does not penetrate the bloodstream but only remains in the gastrointestinal tract where it multiplies and cause severe water loss from the body.
Humans become infected with V. cholerae after consuming food or water that is contaminated with the feaces of infected patients or carriers. Heavy rainfall and floods can also help in spreading the pathogen in places where these events occur. Vegetables contaminated with water containing feaces of infected persons or carriers including fishes from contaminated waters can also spread the disease in human population. Cholera is a serious global public health menace, and it occurs frequently in regions with inadequate water supply and proper sewage treatment facilities.
PATHOGENESIS OF VIBRIO CHOLERAE INFECTION
V. cholerae is a water-borne pathogen that is acquired by humans through the feacal-oral route. Human infection with V. cholerae (serotypes O1 and O139) is initiated following the ingestion of food or water containing significant amount of V. cholerae (usually 108-109 cells). When the mode of entry of V. cholerae into the human host is via food, fewer Vibrio cells (104) are required to initiate an infection. This is because food gives protection to the pathogen against the acidity of the stomach. But when the mode of invasion is water, more V. cholerae cells (1010) will be needed to cause infection because the acidity of the human stomach prevents colonization of the microbe. Upon entry V. cholerae attaches to the epithelial cells of the small intestine using its surface pili and fimbriae.
V. cholerae colonizes the intestinal tract and begins multiplication. As the pathogen multiplies, it starts to produce cholera toxins (CT) which are the main factors that drive V. cholera pathogenicity, and thus responsible for cholera. Cholera toxin is an endotoxin that acts on the epithelial cells of the intestinal tract, and it is solely responsible for the loss of fluid and electrolytes which is associated with the disease. Cholera unlike other bacterial disease is an infection that has biochemical stimulation in that, CT secretion causes an increase in the activity of an enzyme (adenylate cyclase) which inhibits water absorption in the intestinal tract. CT has two subunits known as subunit A and subunit B.
While subunit A activates adenylate cyclase enzyme which increases intestinal levels of cAMP, subunit B binds specifically to the receptors on intestinal mucosa. Binding of subunit B to the receptors of the epithelial cells allow subunit A to enter the intestinal cells. CT activates adenylate cyclase enzymes in the epithelial cells of the intestinal mucosa, and this leads to increase in the level of intracellular cAMP (cyclic adenosine monophosphate). Increase in the concentration of cAMP inhibits the absorption of sodium ions (Na+) by the villi of the small intestine and chloride (Cl–) secretion is increased by crypt cells in the lumen. Generally, the secretion of H20, Na+, K+, Cl–, and HCO3– into the lumen of the small intestine increases on a large scale, and because of this development, there is passive secretion of water by osmotic force, and this generates the watery, diarrheal stool (known as rice-water stool) that is characteristic of cholera.
The patients loses enormous amount of electrolytes and body fluids because of the activation of adenylate cyclase enzyme by CT which culminates to hypersecretion of water and chloride ions and the inhibition of sodium ions in the gut. The incubation of V. cholerae is usually 1-3 days before symptoms including abdominal cramp, fever, vomiting and watery diarrhea begins to manifest. On average, an individual suffering from cholera can lose up to 15 liters of fluid during the period of the infection. Uncontrolled loss of fluids and electrolyte from the body can result in death.
NET EFFECT OF V. CHOLERAE INFECTION IN THE HUMAN BODY
The net effect of cholera in human hosts can be summarized as follows:
- Secretion of electrolytes from the body via vomiting.
- Impairment of sodium ions (Na+).
- Impairment of chloride ions (Cl–).
- Loss of excess bicarbonate ions (HCO–).
- Excessive fluid loss from the body via vomiting and watery stool.
- Acid imbalance in the gastrointestinal (GIT).
LABORATORY DIAGNOSIS OF VIBRIO CHOLERAE INFECTION
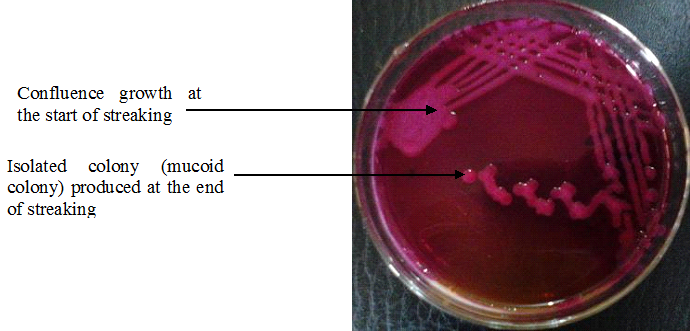
The most important specimen for the laboratory diagnosis of cholera is feaces. Feacal samples are obtained from infected patients for culture and microscopy. V. cholerae is motile and possess a single polar flagellum at one end. V. cholerae grows best in alkaline medium (pH 8.0) that inhibits the growth of other Gram-negative bacteria. Feacal specimens must be transported without delay in Cary-Blair transport medium and cultured in selective media for V. cholerae.Theselective media for the culture of V. cholerae is thiosulphate-citrate bile salt sucrose (TCBS) agar (Figure 1).
V. cholerae can also grow well on other common laboratory media including MacConkey agar and blood agar. V. cholerae also grows rapidly in peptone water (an alkaline medium). The alkalinity of peptone water/agar suppresses the growth of intestinal commensals in the stool specimen. Growth from peptone water should be examined microscopically (i.e. wet preparation), and Gram stained. Colonies growing on TCBS media should be subcultured onto nutrient agar plates before serotyping. Cultures from nutrient agar plates should be serotyped using specific V. cholerae antisera.
IMMUNITY TO VIBRIO CHOLERAE INFECTION
Natural infection with V. cholerae provides long-lasting protection against cholera. Circulating antibodies including IgG and IgA are usually produced and detected against several cholera antigens including the flagella (H) and somatic cell wall (O) antigens, and these are believed to confer some level of immunity against a re-infection.
The acidity of the gastrointestinal tract, motility of the GIT and the intestinal mucus also provide some level of nonspecific protection against gut colonization by V. cholerae. Though an initial attack by cholera provides some level of immunity, the degree and length of protection is still unfathomed. Vaccines are also available against the O1 and O139 serotypes of V. cholerae; however, these vaccines only confer short and variable immunity.
TREATMENT OF VIBRIO CHOLERAE INFECTION
Oral rehydration isthe primary treatment for cholera, and effective solutions can be made by mixing salt, sugar and water which is then administered to the sufferer. Cholera treatment is solely dependent on the immediate replacement of the lost body fluid and electrolytes through the intravenous or oral administration of glucose solutions with near physiologic concentrations of sodium and chloride ions.
Rehydration of lost body fluids should continue until the diarrhea associated with the disease come to an end. Antibiotics are only used in cholera treatment as a secondary treatment measure to fluid and electrolyte replacement. Though resistance to some commonly available antibiotics abound, tetracycline and doxycycline are usually administered orally to contain the profuse stooling during infection and to minimize the amount of Vibrio cells shed in stool.
Sulphamethoxazole-trimethoprim and erythromycin can be used in pregnant women. Mortality rate in cholera endemic areas can be reduced below 1% during outbreaks if effective fluid and electrolyte replacement is put in place without delay. Oral rehydration therapies for cholera treatment are available in exact formulars, and only require a given volume of water for dilution prior to usage.
PREVENTION AND CONTROL OF VIBRIO CHOLERAE INFECTION
Public health education and improvement of public water supply, sewage treatment, sanitation and food handling are critical to the control and prevention of cholera especially in countries where the disease is endemic. People travelling to cholera endemic regions should pay close attention to their personal hygiene, and ensure that they do not eat or drink untreated water or food.
Education of mothers, caregivers, and medical practitioners including medical students and health workers in rural areas of developing countries on the proper dosage of oral rehydration is also important to contain the infection when it occurs. This will go a long way in reversing the infant mortality rate of cholera in developing countries.
OTHER SPECIES OF VIBRIO
- Vibrio mimicus: Vibrio mimicus is an uncommon Vibrio species that causes watery diarrhea and extra-intestinal infections involving wounds, soft tissues and the ear.
- Vibrio parahaemolyticus: V. parahaemolyticus is found in brackish saltwater; when the organism is ingested by the users of such water, it causes gastrointestinal illness. The organism is mainly ingested via the feacal-oral-route; and it can also be ingested by eating raw or undercooked seafood such as oysters.
- Vibrio vulnificus: Vibrio vulnificus is a virulent organism that causes acute gastroenteritis, necrotizing wound infections and invasive septocaemia.
- Vibrio damsela: Vibrio damsel is notorious for causing wound infection; and infection usually occurs through the consumption of contaminated seafood or exposure of a wound to contaminated water (which is the natural habitat of the organism). The elderly and young children are commonly infected with the organism. V. damsela rarely cause septicemia and gastroenteritis.
- Vibrio hollisae: Vibrio hollisae was reclassified in 2003 as Grimontia hollisae based on phylogenetic evidence. It is the only pathogenic species in the family, Vibronaceae that does not grow on thiosulfate-citrate-bile salts-sucrose agar (TCBS), which is a known selective media for the isolation of pathogenic Vibrio species. V. hollisae now G. hollisae primarily cause gastroenteritis in humans.
- Vibrio fluvialis: Vibrio fluvialis can be found in salt waters globally and it has the potential to infect both humans and a variety of crustaceans. It is widely considered to be an emerging pathogen with the potential to have a significant impact on public health. V. fluvialis causes diarrhea in humans.
- Vibrio alginolyticus: – V. alginolyticus isanuncommon Vibrio species that is found in the marine habitat. And it is medically important because it causes otitis and wound infection in humans. V. alginolyticus is a natural host of estuarine and coastal waters and some seafood. This organism is considered a threat to public health because it is an emerging foodborne pathogen.
References
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA. Pp. 248-260.
Madigan M.T., Martinko J.M., Dunlap P.V and Clark D.P (2009). Brock Biology of microorganisms. 12th edition. Pearson Benjamin Cummings Publishers. USA. Pp.795-796.
Prescott L.M., Harley J.P and Klein D.A (2005). Microbiology. 6th ed. McGraw Hill Publishers, USA. Pp. 296-299.
Ryan K, Ray C.G, Ahmed N, Drew W.L and Plorde J (2010). Sherris Medical Microbiology. Fifth edition. McGraw-Hill Publishers, USA.
Singleton P and Sainsbury D (1995). Dictionary of microbiology and molecular biology, 3rd ed. New York: John Wiley and Sons.
Talaro, Kathleen P (2005). Foundations in Microbiology. 5th edition. McGraw-Hill Companies Inc., New York, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.