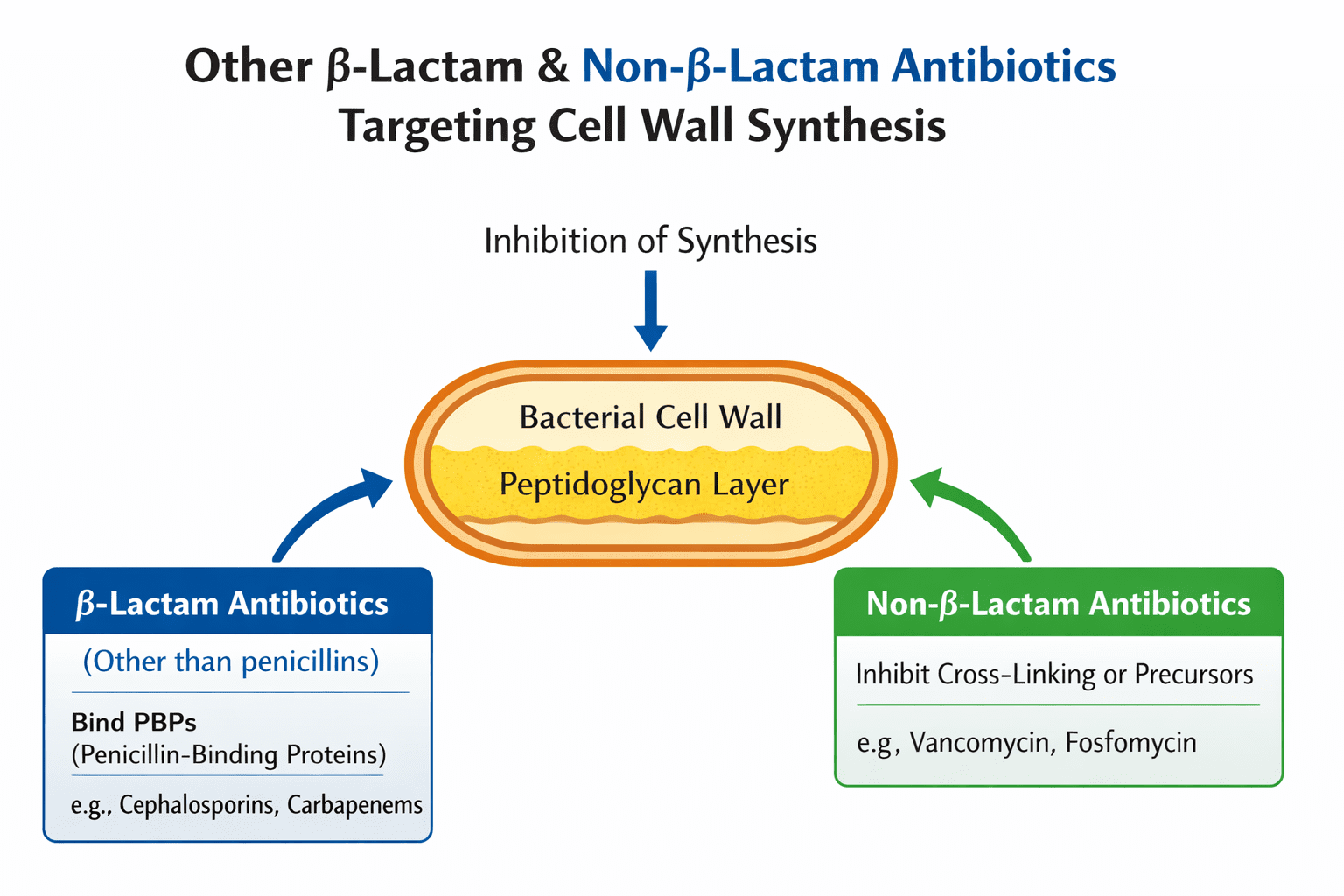
Aside from penicillins and cephalosporins, several other β-lactam and non-β-lactam antibiotics have been developed and are widely employed in clinical practice to manage bacterial infections, particularly those caused by multidrug-resistant pathogens. Penicillins and cephalosporins remain the most familiar and frequently used β-lactam antibiotics; however, the escalating prevalence of resistant bacterial strains has necessitated the development of additional antibiotic classes with enhanced activity and broader antibacterial spectra. These antibiotics primarily function as inhibitors of bacterial cell wall synthesis, a process that is essential for bacterial survival and proliferation. Cell wall biosynthesis, particularly the formation of peptidoglycan, is unique to bacteria and absent in human cells, which confers a high degree of selective toxicity to these drugs. By targeting the enzymes and pathways responsible for peptidoglycan assembly, these antibiotics compromise cell wall integrity, ultimately leading to bacterial lysis and death.
The development of these additional β-lactams and non-β-lactams reflects a combination of structural innovation, improved β-lactamase stability, and the ability to target resistant organisms that are no longer effectively treated with conventional penicillins or cephalosporins. Structurally, many of these drugs retain the β-lactam ring essential for binding to penicillin-binding proteins (PBPs), but they often include modifications that allow them to evade enzymatic degradation, expand their spectrum, or enhance their affinity for multiple PBPs. Non-β-lactam antibiotics, while structurally distinct, achieve a similar outcome by interfering with the biosynthesis of peptidoglycan through alternative mechanisms, such as blocking the transport of precursors or binding directly to peptidoglycan subunits.
These antibiotics exhibit a variety of pharmacological and clinical characteristics, yet all converge on the common goal of disrupting bacterial cell wall synthesis. They differ in their spectrum of activity, pharmacokinetics, clinical indications, and toxicity profiles, which influence their selection for specific infections. Many of these drugs are reserved for severe or complicated infections, often in hospital settings, where multidrug-resistant organisms are prevalent. The judicious use of these agents is critical to preserve their efficacy, as misuse can accelerate the emergence of resistance mechanisms, such as β-lactamase production, target site modifications, or altered permeability.
Below is a summary of key β-lactam and non-β-lactam antibiotics:
- Carbapenems (e.g., imipenem, meropenem, ertapenem): Possess the broadest spectrum of activity among β-lactams, effective against Gram-positive, Gram-negative, and anaerobic bacteria. Clinically used for severe infections caused by multidrug-resistant pathogens, including extended-spectrum β-lactamase (ESBL)-producing organisms.
- Monobactams (e.g., aztreonam): Target Gram-negative bacteria specifically and are particularly useful in patients with penicillin or cephalosporin allergies due to minimal cross-reactivity. Used to treat urinary tract infections, bloodstream infections, and pneumonia caused by susceptible Gram-negative pathogens.
- Cephamycins (e.g., cefotetan, cefoxitin, cefmetazole): Structurally related to cephalosporins but with enhanced stability against β-lactamases and broader activity, including anaerobes. Indicated for intra-abdominal infections, gynecological infections, and surgical prophylaxis.
- Glycopeptides (e.g., vancomycin): Non-β-lactam antibiotics that inhibit peptidoglycan synthesis by binding to D-Ala-D-Ala termini of precursors, primarily effective against Gram-positive bacteria. Used in severe infections caused by methicillin-resistant Staphylococcus aureus (MRSA), enterococcal infections, and Clostridioides difficile colitis.
- Bacitracin: Polypeptide antibiotic that interferes with the transport of peptidoglycan precursors, mainly active against Gram-positive bacteria. Its systemic use is limited due to toxicity; primarily applied topically in ointments, creams, and ophthalmic formulations.
These antibiotics demonstrate that effective disruption of bacterial cell wall synthesis can be achieved through multiple structural and mechanistic strategies. While β-lactams target PBPs to inhibit the transpeptidation reactions essential for cross-linking peptidoglycan, non-β-lactams such as glycopeptides and bacitracin prevent the incorporation or transport of peptidoglycan precursors. The choice of agent depends on several factors, including the pathogen’s susceptibility profile, the site of infection, patient-specific considerations (such as allergies or renal function), and the potential for adverse effects.
The continued evolution of bacterial resistance emphasizes the importance of these alternative β-lactams and non-β-lactams in clinical practice. By extending the therapeutic options beyond penicillins and cephalosporins, they provide clinicians with critical tools to manage infections that would otherwise be difficult or impossible to treat. However, their use must be guided by careful antimicrobial stewardship, susceptibility testing, and consideration of local resistance patterns to maintain their effectiveness for future generations of patients.
Carbapenems
Carbapenems, including imipenem, meropenem, ertapenem, and doripenem, represent one of the most potent groups of β-lactam antibiotics available. Structurally, they share the β-lactam ring core characteristic of penicillins and cephalosporins, but possess modifications that confer remarkable stability against most β-lactamases, including extended-spectrum β-lactamases (ESBLs). This feature allows carbapenems to retain activity against a broad range of Gram-positive, Gram-negative, and anaerobic bacteria, positioning them as drugs of choice for severe, multidrug-resistant infections.
Mechanistically, carbapenems inhibit bacterial cell wall synthesis by binding to penicillin-binding proteins (PBPs).PBPs are enzymes responsible for the final cross-linking of the peptidoglycan matrix, a process known as transpeptidation. By acylating the active site of these enzymes, carbapenems prevent cross-link formation, compromising cell wall integrity, leading to osmotic lysis and bacterial death. Their high affinity for multiple PBPs, including those not targeted efficiently by other β-lactams, accounts for their exceptional potency and broad spectrum of activity.
Clinically, carbapenems are used to treat complicated intra-abdominal infections, hospital-acquired pneumonia, septicemia, and infections caused by multidrug-resistant Gram-negative bacilli, including Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa. Their activity against anaerobes, including Bacteroides fragilis, makes them particularly useful in polymicrobial infections. Importantly, carbapenems are often reserved as last-line therapy to delay the emergence of resistance.
Resistance to carbapenems, though relatively rare, is a growing concern. The primary mechanism involves the production of carbapenemases, such as KPC (Klebsiella pneumoniae carbapenemase) and NDM-1 (New Delhi metallo-β-lactamase), which hydrolyze the β-lactam ring. Additionally, mutations that reduce outer membrane permeability or upregulate efflux pumps can confer carbapenem resistance. The clinical implications are significant, as infections with carbapenem-resistant organisms are associated with high morbidity and mortality, underscoring the necessity for judicious use and ongoing surveillance.
Monobactams
Monobactams are a unique subclass of β-lactam antibiotics characterized by a monocyclic β-lactam structure, distinguishing them from the bicyclic penicillins and cephalosporins. Aztreonam is the most widely used monobactam and is particularly effective against aerobic Gram-negative bacteria, including Pseudomonas aeruginosa.
The mechanism of action mirrors that of other β-lactams: inhibition of PBPs prevents cross-linking of peptidoglycan layers, weakening the bacterial cell wall and causing cell death. However, monobactams exhibit minimal activity against Gram-positive bacteria and anaerobes, largely due to their inability to penetrate the thicker peptidoglycan layers and their specificity for Gram-negative PBPs.
A key clinical advantage of aztreonam is its safety in patients with penicillin allergies. Because its monocyclic structure is immunologically distinct from penicillins and cephalosporins, cross-reactivity is extremely low. This property allows clinicians to treat serious Gram-negative infections in penicillin-allergic patients without risking hypersensitivity reactions.
Monobactams are primarily indicated for urinary tract infections, bloodstream infections, and lower respiratory tract infections caused by susceptible Gram-negative pathogens. Resistance mechanisms are similar to those seen in other β-lactams and include production of β-lactamases, especially ESBLs, and mutations in outer membrane porins, which reduce drug uptake. Despite these challenges, aztreonam remains a vital therapeutic option in the antimicrobial arsenal, especially in the era of rising multidrug resistance.
Cephamycins
Cephamycins are β-lactam antibiotics structurally related to cephalosporins but with notable modifications that enhance their spectrum of activity and β-lactamase stability. Examples include cefotetan, cefoxitin, and cefmetazole. Naturally derived from Streptomyces species, cephamycins can now be synthesized industrially, allowing for consistent pharmacological properties.
Mechanistically, cephamycins inhibit cell wall synthesis through PBP binding and subsequent inhibition of peptidoglycan cross-linking. Their enhanced stability against β-lactamases, particularly those produced by Gram-negative bacteria, allows them to retain activity where early-generation cephalosporins fail. They are especially effective against anaerobic organisms, making them suitable for intra-abdominal and gynecological infections.
Clinically, cephamycins are used in surgical prophylaxis, intra-abdominal infections, and infections caused by β-lactamase-producing Enterobacteriaceae. Their broader spectrum compared to cephalosporins allows them to fill a therapeutic niche between traditional cephalosporins and carbapenems. However, resistance can still emerge via extended-spectrum β-lactamases, efflux pumps, or alterations in PBPs, highlighting the need for susceptibility testing before clinical use.
Glycopeptides
Glycopeptides, such as vancomycin, are non-β-lactam antibiotics that inhibit bacterial cell wall synthesis by a mechanism distinct from β-lactams. Produced by Streptomyces species, vancomycin binds to the D-Ala-D-Ala termini of peptidoglycan precursors, preventing transglycosylation and transpeptidation reactions necessary for cell wall elongation. Unlike β-lactams, glycopeptides do not acylate PBPs directly but sterically hinder substrate availability.
Glycopeptides are primarily active against Gram-positive bacteria, including Staphylococcus aureus, Streptococcus species, and Enterococcus species. Their inability to penetrate the outer membrane of Gram-negative bacteria limits their use against such pathogens. Clinically, vancomycin is essential for treating methicillin-resistant S. aureus (MRSA) infections, severe Clostridioides difficile infections, and endocarditis caused by resistant Gram-positive organisms.
Resistance, notably vancomycin-resistant enterococci (VRE), has emerged through the acquisition of genes such as vanA and vanB, which modify the D-Ala-D-Ala terminus to D-Ala-D-Lac, reducing vancomycin binding affinity. The rise of such resistance underscores the need for novel glycopeptide derivatives and combination therapies to maintain clinical efficacy.
Bacitracin
Bacitracin is a polypeptide antibiotic produced by the bacterium Bacillus licheniformis. Unlike β-lactam antibiotics such as penicillins and cephalosporins, bacitracin does not contain a β-lactam ring but still interferes with bacterial cell wall synthesis. Due to its relatively high toxicity when administered systemically, bacitracin is used almost exclusively as a topical antimicrobial agent. It is commonly incorporated into ointments, creams, and ophthalmic preparations for the prevention and treatment of localized bacterial infections.
The antibacterial activity of bacitracin results from its interference with an early stage of peptidoglycan biosynthesis. Specifically, bacitracin inhibits the dephosphorylation of bactoprenol (also known as undecaprenyl pyrophosphate), a lipid carrier molecule embedded in the bacterial cytoplasmic membrane. Bactoprenol plays a crucial role in transporting peptidoglycan precursor units from the cytoplasm to the exterior of the cell membrane, where they are incorporated into the growing cell wall structure. By preventing the recycling of bactoprenol, bacitracin effectively blocks the translocation of these precursors, thereby halting peptidoglycan assembly. This disruption weakens the structural integrity of the bacterial cell wall and ultimately leads to bacterial cell death, particularly in actively dividing cells.
Bacitracin exhibits strong activity against many Gram-positive bacteria, including species of Staphylococcus and Streptococcus. However, it has limited effectiveness against Gram-negative organisms because the outer membrane of these bacteria acts as a permeability barrier that prevents the antibiotic from reaching its target. Clinically, bacitracin is widely used in topical formulations for the treatment of minor skin infections, cuts, abrasions, and burns, as well as for prophylaxis in surgical wounds. It is also frequently combined with other antibiotics, such as neomycin or polymyxin B, to broaden the antimicrobial spectrum in topical preparations.
Systemic administration of bacitracin is generally avoided because of its potential nephrotoxicity, which can lead to kidney damage. Nevertheless, its topical use remains highly valuable due to its effectiveness and low risk of systemic absorption. Although bacterial resistance to bacitracin is relatively uncommon, it can occur through mechanisms such as efflux pumps or alterations in enzymes involved in bactoprenol recycling. Bacitracin remains an important antimicrobial agent for localized infections, particularly when used in combination therapies that enhance antibacterial coverage while minimizing systemic toxicity.
References
Ashutosh Kar (2008). Pharmaceutical Microbiology, 1st edition. New Age International Publishers: New Delhi, India.
Axelsen P. H (2002). Essentials of Antimicrobial Pharmacology. Humana Press, Totowa, NJ.
Balfour H. H (1999). Antiviral drugs. N Engl J Med, 340, 1255–1268.
Beck R.W (2000). A chronology of microbiology in historical context. Washington, D.C.: ASM Press.
Chemotherapy of microbial diseases. In: Chabner B.A, Brunton L.L, Knollman B.C, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. New York, McGraw-Hill; 2011.
Chung K.T, Stevens Jr., S.E and Ferris D.H (1995). A chronology of events and pioneers of microbiology. SIM News, 45(1):3–13.
Courvalin P, Leclercq R and Rice L.B (2010). Antibiogram. ESKA Publishing, ASM Press, Canada.
Denyer S.P., Hodges N.A and Gorman S.P (2004). Hugo & Russell’s Pharmaceutical Microbiology. 7th ed. Blackwell Publishing Company, USA. Pp.152-172.
Dictionary of Microbiology and Molecular Biology, 3rd Edition. Paul Singleton and Diana Sainsbury. 2006, John Wiley & Sons Ltd. Canada.
Drusano G.L (2007). Pharmacokinetics and pharmacodynamics of antimicrobials. Clin Infect Dis, 45(suppl):89–95.
Engleberg N.C, DiRita V and Dermody T.S (2007). Schaechter’s Mechanisms of Microbial Disease. 4th ed. Lippincott Williams & Wilkins, Philadelphia, USA.
Finch R.G, Greenwood D, Norrby R and Whitley R (2002). Antibiotic and chemotherapy, 8th edition. Churchill Livingstone, London and Edinburg.
Ghannoum MA, Rice LB (1999). Antifungal agents: Mode of action, mechanisms of resistance, and correlation of these mechanisms with bacterial resistance. Clin Microbiol Rev, 12:501–517.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.