Methicillin-resistant Staphylococcus aureus (MRSA) is a type of bacterium that has become resistant to many antibiotics, particularly beta-lactams such as methicillin, oxacillin, penicillin, and amoxicillin. First identified in the early 1960s, MRSA has emerged as a serious public health concern worldwide due to its capacity to cause both hospital-acquired and community-acquired infections that are difficult to treat. It exemplifies the growing challenge of antimicrobial resistance (AMR), which the World Health Organization (WHO) considers one of the top ten global public health threats.
The Biology of MRSA
Staphylococcus aureus is a common bacterium found on the skin and in the noses of up to 30% of healthy individuals. While often harmless, it can cause infections when it enters the body through cuts, wounds, or medical devices. MRSA is a strain of S. aureus that has acquired the mecA gene, which encodes an altered penicillin-binding protein (PBP2a). This protein renders beta-lactam antibiotics ineffective by preventing them from binding to bacterial cell walls, a mechanism these drugs typically use to kill the bacteria.
Types of MRSA
There are two major types of MRSA infections:
- Healthcare-associated MRSA (HA-MRSA): These infections occur in hospitals and other healthcare settings, typically affecting patients with weakened immune systems, surgical wounds, or invasive devices like catheters. HA-MRSA is often responsible for bloodstream infections, pneumonia, surgical site infections, and sepsis.
2. Community-associated MRSA (CA-MRSA): This type affects healthy individuals outside healthcare facilities and is usually transmitted through close physical contact or shared personal items such as towels or sports equipment. CA-MRSA often causes skin and soft tissue infections like boils, abscesses, and cellulitis, but can sometimes lead to more severe complications like necrotizing pneumonia.
Epidemiology of MRSA
MRSA infections have spread globally, with significant variation in prevalence across regions. In the United States, the Centers for Disease Control and Prevention (CDC) estimate that MRSA is responsible for about 10,000 deaths annually. In Europe and parts of Asia and Africa, MRSA remains a major cause of hospital infections, though concerted efforts in surveillance and infection control have led to some reduction in prevalence in recent years.
The emergence of livestock-associated MRSA (LA-MRSA), particularly the ST398 strain found in pigs and other farm animals, has raised further concern about zoonotic transmission and the role of antibiotic use in agriculture in fueling resistance.
Transmission and Risk Factors of MRSA
MRSA spreads primarily through direct contact with an infected wound or by touching contaminated surfaces. Risk factors include:
- Recent hospitalization or surgery
- Living in crowded settings (e.g., prisons, military barracks)
- Participation in contact sports
- Sharing personal items
- Poor hygiene
- Use of invasive medical devices
Healthcare workers and caregivers are also at high risk due to their frequent contact with patients and contaminated surfaces.
Clinical Manifestations of MRSA
MRSA infections range from mild skin conditions to life-threatening diseases. Common symptoms include:
- Red, swollen, and painful skin lesions
- Pus or drainage from wounds
- Fever and chills (in systemic infections)
- Shortness of breath (in pneumonia)
- Confusion or disorientation (in bloodstream infections or sepsis)
Prompt diagnosis and treatment are critical to prevent complications due to MRSA infections.
Diagnosis and Treatment
Diagnosis involves collecting samples from the site of infection (e.g., wound, blood, or sputum) and performing laboratory tests, including culture and antibiotic susceptibility testing. Rapid molecular tests can also detect the mecA gene.
Treating MRSA can be challenging due to its resistance profile. However, several antibiotics remain effective against MRSA, including:
- Vancomycin (often the first-line treatment for severe infections)
- Linezolid
- Daptomycin
- Clindamycin
- Trimethoprim-sulfamethoxazole
- Tetracyclines (e.g., doxycycline)
The choice of antibiotic depends on the site and severity of the infection, patient factors, and local resistance patterns. Surgical drainage may be necessary for abscesses or deep-seated infections.
Prevention and Control of MRSA Infection
Preventing MRSA requires a multifaceted approach:
- In healthcare settings: Rigorous hand hygiene, use of personal protective equipment (PPE), environmental cleaning, contact precautions, and antibiotic stewardship programs are essential.
- In the community: Good personal hygiene, proper wound care, and avoiding sharing personal items can reduce transmission.
- In agriculture: Reducing the use of antibiotics in livestock and improving animal husbandry practices can help curb the spread of LA-MRSA.
Research and Future Directions
Research is ongoing to develop new antibiotics, vaccines, and diagnostic tools to combat MRSA. Phage therapy, antimicrobial peptides, and immunotherapy are also being explored as alternative treatment strategies. Strengthening global surveillance systems and promoting coordinated responses to AMR threats remain priorities.
MRSA represents a formidable challenge in the era of antimicrobial resistance. Its ability to spread rapidly and cause severe infections in both hospital and community settings makes it a critical focus for public health efforts. Combating MRSA requires continued vigilance, responsible antibiotic use, enhanced infection control practices, and sustained investment in research and innovation. Only through a comprehensive One Health approach – integrating human, animal, and environmental health – can we effectively address the growing threat posed by MRSA and similar resistant pathogens.
Methicillin resistant Staphylococcus aureus (MRSA) as aforesaid is defined as a pathogenic Staphylococcus aureus strain that is resistant to methicillin and other beta-lactam antibiotics such as oxacillin. MRSA is a highly contagious strain of the staphylococci bacteria, which cause a number of infections in human population. MRSA strain cause community-acquired methicillin-resistant S. aureus (CA-MRSA) infection and hospital-acquired methicillin-resistant S. aureus (HA-MRSA) infections; and their occurrence have been reported in many parts of the world. MRSA cause a wide variety of deep tissue infections, including osteomyelitis, arthritis, endocarditis, skin infections, and pneumonia.
Methicillin resistance was found in the strains of Staphylococcus aureus, soon after the introduction of methicillin into clinical medicine in the 1960s. Methicillin is a beta-lactam antibiotic that bears similar structure with the penicillins because they both contain beta-lactam ring in their structure. Irrespective of their potent antimicrobial activity, methicillin resistance was found in some strains of Staphylococcus aureus, and MRSA cause significant infections in both the hospital and community settings.
The resistance of Staphylococcus aureusto the antibiotic methicillin has been associated to a chromosomal mecA gene that specifies the production of an abnormal penicillin-binding-protein (PBP) in the organism. Penicillin-binding-proteins (PBPs) are membrane-bound enzymes that catalyze the transpeptidation reaction that is necessary for cross-linkage of peptidoglycan layer in both Gram positive and Gram negative bacteria, and this transpeptidation reaction is critical for the formation of a solid cell wall in bacteria.
MRSA also include S. aureus strains that are oxacillin resistant and not only methicillin resistant. MRSA and/or oxacillin-resistant S. aureus strains are multiply resistant to some commonly available antibiotics including erythromycin, clindamycin, tetracycline, cephalosporins and carbapenems. However, MRSA strains are usually susceptible to glycopeptides, vancomycin and teicoplanin. Thus, these antibiotics (i.e. teicoplanin, glycopeptides and vancomycin) are the only drug of choice for the treatment of severe infections due to MRSA.
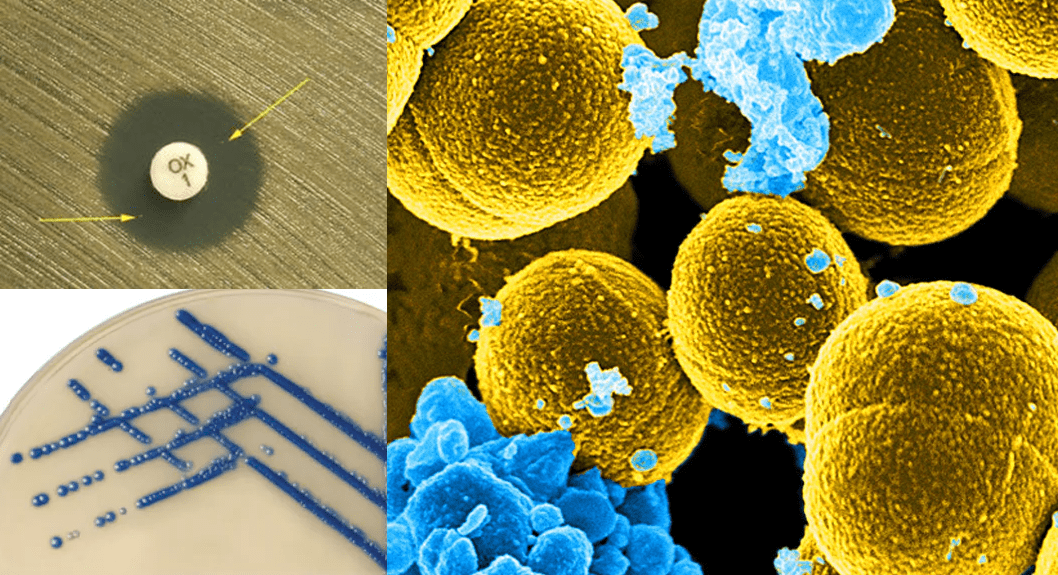
Some strains of MRSA also remain susceptible to some non-beta-lactam agents including fluoroquinolones, sulphamethoxazole-trimethoprim, and gentamicin. But reports of MRSA strains with decreased susceptibility to vancomycin (minimum inhibitory concentration [MIC], >8 mg/ml) have been observed in some MRSA strains. The Clinical Laboratory Standard Institute (CLSI), formerly National Committee for Clinical Laboratory Standards (NCCLS) recommends the use of oxacillin disk (1 µg or 5 µg) or methicillin disk for the screening of S. aureus isolates for the presence or detection of resistance to methicillin/oxacillin (Table 1).
Table 1 shows the antibiotic breakpoints for the phenotypic screening of S. aureus isolates for the presence of mecA genes. Nevertheless, the accurate detection of oxacillin/methicillin resistance in potential pathogenic S. aureus strains suspected to be MRSA strains can be difficult due to the presence of two subpopulations of MRSA isolates (i.e. MRSA heterosusceptible strains and MRSA heteroresistant strain).
While heterosusceptible MRSA strains are susceptible to methicillin/oxacillin, the later (heteroresistant strains) are resistant; and both strains can coexist within a particular culture plate (Figure 1). All S. aureus cells in a culture plate may harbour the genetic information that is responsible for S. aureus resistance to oxacillin/methicillin but only a small number of these cells can actually express the resistance in vitro.
This phenomenon is termed “heteroresistance” and it only occurs in staphylococci that are resistant to penicillinase-stable penicillins such as oxacillin. However, amplification tests like those based on the polymerase chain reaction (PCR) can detect the mecA gene that is responsible for S. aureus resistance to oxacillin/methicillin. PCR gene amplification test and other genotypic tests for MRSA detection helps to confirm oxacillin/methicillin resistance caused by mecA gene in Staphylococcus species.
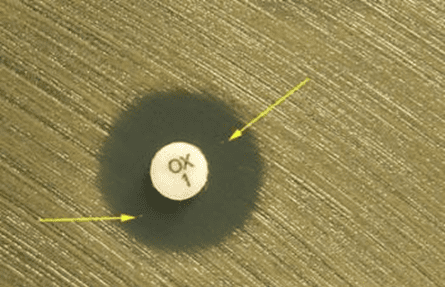
Table 1. MIC and inhibition zone diameter breakpoints for disk diffusion test for MRSA detection
| MICs | Oxacillin susceptible | Oxacillin intermediate | Oxacillin resistant |
| S. aureus | < 2 mg/ml | no intermediate MIC | MIC > 4 mg /ml |
| CoNS* | < 0.25 mg /ml | No intermediate MIC | MIC > 0.5 mg /ml |
| Zone sizes | Oxacillin Susceptible | Oxacillin intermediate | Oxacillin Resistant |
| S. aureus | > 13 mm | 11-12 mm | < 10 mm |
| CoNS* | > 18 mm | no intermediate zone | < 17 mm |
*CoNS = Coagulase negative Staphylococcus aureus
Figure 1 is the surface of a Mueller-Hinton agar plate inoculated with a strain of S. aureus suspected of being methicillin-resistant. Though the zone of inhibition is at the borderline for resistance (18 mm), the presence of small colonies within the zone of inhibition (arrows) indicates the presence of heteroresistant strains of S. aureus. The interpretation here, therefore, is “methicillin-resistant” staphylococci, even though the zone diameter appears to be adequate. The detection of the heteroresistant strains in disk diffusion test indicates that minimum inhibitory concentration (MIC) studies are required to confirm the presence of MRSA strains.
Heteroresistance is a problem for clinical microbiology laboratory personnel who look out for MRSA strains from clinical specimens. This is because S. aureus cells expressing heteroresistance may grow more slowly than the susceptible S. aureus population in a culture; and they are not easily inhibited by oxacillin. Thus, S. aureus isolates being tested against oxacillin, methicillin, or nafcillin should be incubated at 35° C for complete 24 hours incubation before taking the antibiogram and/or culture reading.
The breakpoints for S. aureus are different from those for coagulase-negative staphylococci (CoNS) such as S. epidermidis – which is usually the most common CoNS isolated from clinical samples (Table 1). It is also noteworthy that methicillin-susceptible S. aureus (MSSA) can become MRSA through the acquisition of staphylococcal chromosome cassette mec (SCCmec), which contains mecA gene (the methicillin resistance determinant gene). Gene acquisition of SCCmec gene is usually through genetic transfer mechanisms such as conjugation, transduction or transformation.
References
Ashutosh Kar (2008). Pharmaceutical Microbiology, 1st edition. New Age International Publishers: New Delhi, India.
Axelsen P.H (2002). Essentials of antimicrobial pharmacology. Humana Press, Totowa, New Jersey, USA. Al-Jasser A.M (2006). Extended – Spectrum Beta – Lactamases (ESBLs): A Global Problem. Kuwait Medical Journal, 38(3):171-185.
Bisht R., Katiyar A., Singh R and Mittal P (2009). Antibiotic Resistance – A Global Issue of Concern. Asian Journal of Pharmaceutical and Clinical Research, 2 (2):34-39.
Block S.S (2001). Disinfection, sterilization and preservation. 5th edition. Lippincott Williams & Wilkins, Philadelphia and London.
Cars O and Nordberg P (2005). Antibiotic resistance: The faceless threat. International Journal of Risk & Safety in Medicine, 17 (3/4): 103-110.
Finch R.G, Greenwood D, Norrby R and Whitley R (2002). Antibiotic and chemotherapy, 8th edition. Churchill Livingstone, London and Edinburg.
Livermore D.M (2004). The need for new antibiotics. Clinical Microbiology & Infection, 4(10): 1-9.
Mascaretti O.A (2003). Bacteria versus antibacterial agents: An integrated approach. Washington: ASM Press.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.