Hantaviruses are classified as Category C biological agents, the third-highest priority group of pathogens considered to have potential for bioterrorism. They are medically significant zoonotic pathogens belonging to the family Hantaviridae and the order Bunyavirales. The genus Orthohantavirus contains most hantaviruses pathogenic to humans. Humans are only incidental hosts of the virus. These enveloped, negative-sense single-stranded RNA viruses are primarily maintained in rodent reservoirs and are transmitted to humans mainly through exposure to infected rodent excreta, including urine, feces, and saliva.
Human infection most commonly occurs through inhalation of aerosolized viral particles in contaminated environments. Unlike many other members of the order Bunyavirales, hantaviruses are not arthropod-borne and do not require insect vectors such as mosquitoes or ticks for transmission. Each hantavirus species is typically associated with a specific rodent host, reflecting a close evolutionary relationship between the virus and its reservoir. Most hantaviruses are not transmitted between humans. However, Andes virus in South America has demonstrated limited person-to-person transmission, particularly among close contacts.
Hantavirus infection reminds us how closely environmental health, rodent ecology, and human health are connected. These infections represent an important global public health concern due to their high morbidity and mortality rates, wide geographic distribution, and increasing incidence in regions with intense human-rodent interaction. Environmental disruption, agricultural expansion, urbanization, deforestation, and climate variability have all contributed to increased opportunities for zoonotic spillover. Consequently, hantavirus outbreaks continue to emerge in both endemic and previously unaffected areas.
Two major clinical syndromes are associated with hantavirus infection. In Europe and Asia, hantaviruses predominantly cause hemorrhagic fever with renal syndrome (HFRS), a disease characterized by fever, thrombocytopenia, hemorrhage, hypotension, and acute kidney injury. In contrast, hantavirus pulmonary syndrome (HPS), also referred to as hantavirus cardiopulmonary syndrome (HCPS), occurs mainly in North and South America and is marked by rapidly progressive pulmonary edema, respiratory failure, and cardiovascular collapse. Despite differences in geographic distribution and clinical presentation, both syndromes share a common pathogenic mechanism involving endothelial dysfunction, exaggerated immune activation, and increased vascular permeability.
The pathogenesis of hantavirus disease is largely immune mediated rather than directly cytopathic. Following viral entry, hantaviruses infect endothelial cells lining the vasculature without causing extensive cellular destruction. Instead, activation of immune responses and release of pro-inflammatory cytokines lead to capillary leakage, tissue edema, and multiorgan dysfunction. Severe infections may result in shock, disseminated intravascular coagulation, respiratory failure, or renal impairment depending on the viral species involved.
Since the isolation of Hantaan virus in South Korea in 1978, substantial progress has been made in understanding hantavirus molecular biology, taxonomy, epidemiology, and host-pathogen interactions. Numerous hantavirus species have since been identified worldwide, including Hantaan, Seoul, Puumala, Dobrava-Belgrade, Sin Nombre, and Andes viruses, each associated with distinct reservoir hosts and disease patterns. Advances in molecular diagnostics, particularly reverse transcription polymerase chain reaction (RT-PCR) and serological assays, have improved the accuracy and speed of laboratory diagnosis.
Despite these scientific advances, the management of hantavirus infection remains largely supportive. No universally approved antiviral therapy exists for all hantavirus infections, although ribavirin has demonstrated partial efficacy in selected cases of HFRS when administered early. Likewise, no globally licensed vaccine is currently available for widespread human use, although inactivated vaccines are used in limited settings in parts of Asia and several experimental vaccine candidates remain under investigation.
Consequently, prevention and control strategies continue to rely heavily on minimizing human exposure to infected rodents. Effective measures include rodent population control, environmental sanitation, safe cleaning practices in contaminated areas, occupational protection, and public health education. Surveillance systems and ecological monitoring are also essential for early outbreak detection and risk assessment, particularly in the context of climate change and environmental transformation that may alter rodent population dynamics and disease transmission patterns.
Ongoing research into antiviral agents, vaccine development, immunopathogenesis, and reservoir ecology is critical for reducing the global burden of hantavirus disease. In this regard, a multidisciplinary One Health approach integrating human, animal, and environmental health perspectives remains fundamental for the prevention, surveillance, and control of hantavirus infections worldwide.
Brief history of Hantavirus
The history of hantavirus infection dates back several centuries, although the viral etiology was only identified in the twentieth century. Historical records from China and Russia describe illnesses consistent with hemorrhagic fever accompanied by kidney dysfunction. However, the disease gained major international attention during the Korean War between 1950 and 1953. During the Korean War, more than 3,000 United Nations soldiers developed a severe febrile illness characterized by hemorrhage, renal failure, hypotension, and shock. The condition became known as Korean hemorrhagic fever. The cause remained unknown for many years until 1978, when Korean scientist Ho Wang Lee successfully isolated the causative virus from the striped field mouse, Apodemus agrarius, near the Hantaan River in South Korea. The virus was named Hantaan virus after the river where it was discovered.
The discovery of Hantaan virus marked the beginning of modern hantavirus research. Subsequently, additional hantaviruses were identified across Europe and Asia, including Seoul virus, Puumala virus, and Dobrava-Belgrade virus. These viruses were linked to varying severities of hemorrhagic fever with renal syndrome. A second major milestone occurred in 1993 in the Four Corners region of the southwestern United States, where an outbreak of severe respiratory illness with high mortality affected previously healthy young adults. Investigations by the Centers for Disease Control and Prevention (CDC) identified a novel hantavirus later named Sin Nombre virus. The deer mouse, Peromyscus maniculatus, was identified as the reservoir host.
This outbreak led to recognition of hantavirus pulmonary syndrome, a disease distinct from the renal syndrome observed in Eurasia. Since then, numerous hantaviruses associated with pulmonary disease have been identified in North and South America, including Andes virus, Laguna Negra virus, and Choclo virus. Research over recent decades has improved understanding of hantavirus molecular biology, ecology, immunopathogenesis, and clinical management. However, hantavirus infections continue to cause outbreaks worldwide, particularly in areas with changing ecological conditions.
Biology of Hantavirus
Viral structure of Hantavirus
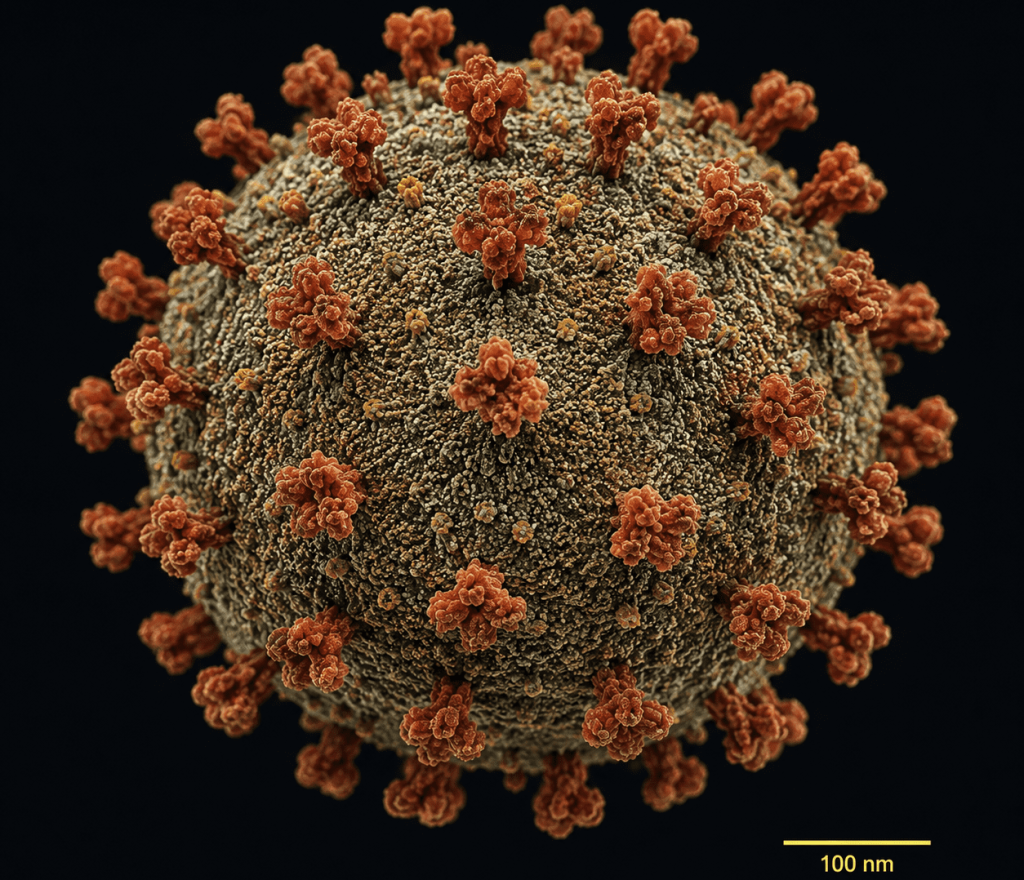
Hantaviruses are enveloped viruses with a spherical or pleomorphic morphology measuring approximately 80-120 nm in diameter (Figure 1). Their genome consists of three segments of single-stranded, negative-sense RNA designated as small (S), medium (M), and large (L) segments. The S segment encodes the nucleocapsid (N) protein, which encapsidates viral RNA and plays a role in viral replication and immune modulation. The M segment encodes the glycoprotein precursor that is cleaved into two envelope glycoproteins, Gn and Gc, which are essential for viral attachment and entry into host cells. The L segment encodes the viral RNA-dependent RNA polymerase responsible for transcription and replication. The viral envelope is derived from host cell membranes and contains embedded glycoprotein spikes that facilitate interaction with host cell receptors. Hantaviruses are relatively stable in the environment under cool and humid conditions but are susceptible to heat, detergents, and disinfectants.
Replication cycle of Hantavirus
The hantavirus replication cycle begins with attachment of viral glycoproteins to receptors on host endothelial cells, macrophages, and dendritic cells. Integrins, particularly β3 integrins, are important receptors involved in viral entry. Following attachment, the virus enters cells through endocytosis. Acidification within endosomes triggers fusion of the viral envelope with endosomal membranes, allowing release of ribonucleoprotein complexes into the cytoplasm. Transcription and replication occur in the cytoplasm using the viral RNA polymerase. Viral proteins are synthesized by host ribosomes, and glycoproteins undergo maturation in the Golgi apparatus. Newly assembled virions bud into the Golgi and are subsequently transported to the cell surface for release. Unlike many cytopathic viruses, hantaviruses generally do not directly destroy infected endothelial cells. Instead, disease manifestations are largely due to immune-mediated mechanisms and vascular dysfunction.
Reservoir hosts for Hantavirus
Rodents are the principal reservoirs of hantaviruses. Each hantavirus species is typically associated with a specific rodent host species. These rodents usually develop persistent asymptomatic infections and shed virus in urine, feces, and saliva for prolonged periods.
Some of the major reservoir hosts and their specific virus are:
- Hantaan virus: This is associated with the striped field mouse.
- Seoul virus: This is associated with the Norway rat.
- Puumala virus: This is associated with the bank vole.
- Sin Nombre virus: This is associated with the deer mouse (Figure 2).
- Andes virus: This is associated with the long-tailed pygmy rice rat.

Major human pathogenic hantaviruses
Old World Hantaviruses
These viruses are found mainly in Europe and Asia and typically cause hemorrhagic fever with renal syndrome. Examples include:
- Hantaan virus
- Seoul virus
- Puumala virus
- Dobrava-Belgrade virus
- Amur virus
New World Hantaviruses
These viruses occur mainly in North and South America and are associated with hantavirus pulmonary syndrome. Examples include:
- Sin Nombre virus
- Andes virus
- Laguna Negra virus
- Black Creek Canal virus
- Choclo virus
Genetic diversity of Hantaviruses
Hantaviruses exhibit remarkable genetic diversity, which is primarily driven by mutation, natural selection, reassortment of genomic segments, and adaptation to different reservoir hosts. As RNA viruses, hantaviruses possess error-prone RNA-dependent RNA polymerases that lack proofreading ability, resulting in frequent genetic mutations during replication. These mutations contribute to the emergence of genetically distinct strains and influence viral evolution, pathogenicity, and host specificity. In addition, reassortment may occur when two related hantaviruses infect the same host cell, allowing exchange of genome segments and generation of novel variants.
Phylogenetic studies have shown that hantavirus evolution is closely associated with the evolution of their rodent hosts, a phenomenon referred to as co-evolution. Most hantaviruses are strongly linked to specific rodent species, and geographic distribution of the virus often mirrors that of the host reservoir. Geographic isolation, ecological differences, and host adaptation contribute significantly to genetic divergence among hantaviruses found in different regions of the world.
Recent molecular investigations have expanded the understanding of hantavirus diversity by identifying hantavirus-like viruses in insectivores such as shrews and moles, as well as in bats. These discoveries suggest that the evolutionary history of hantaviruses is more ancient and complex than previously believed. The presence of diverse hantavirus lineages in multiple mammalian hosts raises concerns about the potential emergence of new zoonotic strains capable of infecting humans.
Pathogenesis of Hantavirus infection
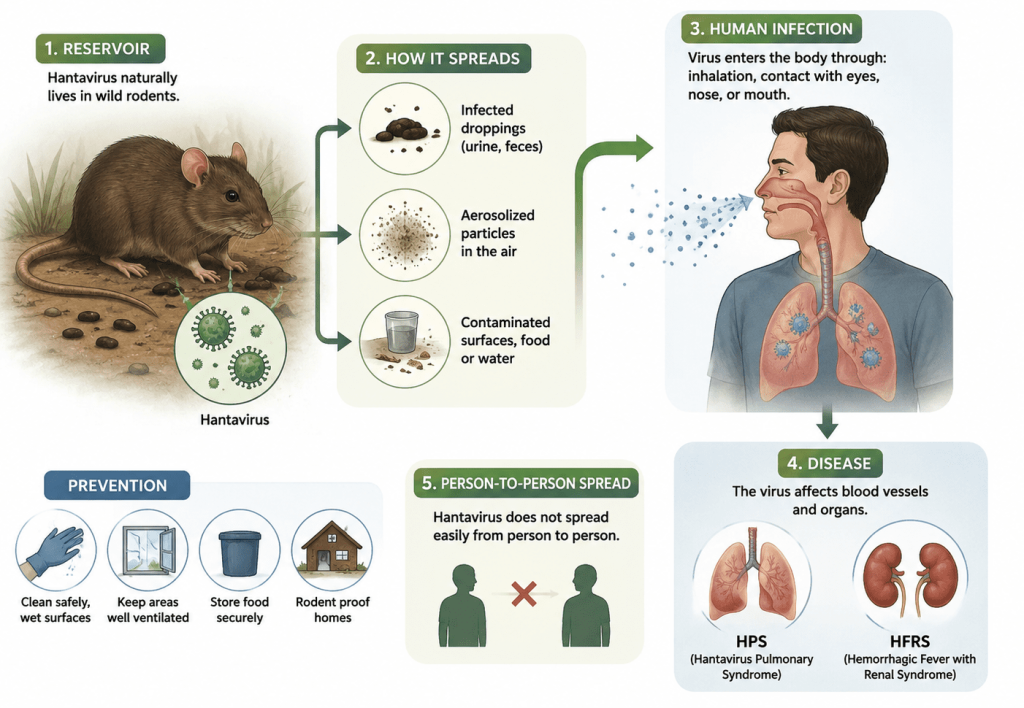
The pathogenesis of hantavirus infection is complex. The virus is spread to humans through rodent droppings and urine (Figure 3). Its pathogenesis usually involves viral replication, endothelial dysfunction, immune activation, and increased vascular permeability. The major stages in the pathogenesis of Hantavirus infections are as follows:
1. Viral entry and dissemination
After inhalation of aerosolized particles usually from reservoir hosts such as rodents (Figure 2), hantaviruses infect respiratory epithelial cells and subsequently spread to endothelial cells lining blood vessels. The virus disseminates systemically through the bloodstream. Endothelial cells are primary targets of infection. Despite widespread infection, cellular destruction is limited. Instead, altered endothelial function results in increased capillary permeability.
2. Immune response
The host immune response plays a central role in disease severity. Infected cells produce cytokines and chemokines that recruit immune cells, including T lymphocytes, macrophages, and natural killer cells. Excessive production of inflammatory mediators such as tumor necrosis factor-alpha, interleukin-6, and interferon-gamma contributes to endothelial activation and vascular leakage. Cytotoxic T-cell responses against infected endothelial cells may exacerbate tissue injury. Elevated cytokine levels correlate with severe disease manifestations.
3. Vascular leakage
The hallmark of hantavirus disease is increased vascular permeability. Leakage of plasma into tissues causes hypotension, edema, hemoconcentration, and shock. In HFRS, vascular leakage predominantly affects the kidneys, leading to acute kidney injury and hemorrhagic manifestations. In HPS, pulmonary capillary leakage causes noncardiogenic pulmonary edema and respiratory failure.
4. Coagulation abnormalities
Thrombocytopenia and coagulation abnormalities are common. Platelet dysfunction and endothelial activation contribute to hemorrhagic complications. Disseminated intravascular coagulation may occur in severe cases of Hantavirus infection.
- Organ involvement
Kidney Involvement: Renal involvement is one of the hallmark features of HFRS. Following infection, hantaviruses primarily affect the vascular endothelium of the kidneys, leading to increased capillary permeability, interstitial edema, and inflammatory cell infiltration. Histopathological findings commonly include interstitial nephritis, acute tubular necrosis, and impaired glomerular filtration. These pathological changes result in significant renal dysfunction characterized by oliguria, elevated serum creatinine, proteinuria, and hematuria. In severe cases, acute kidney injury may develop and require dialysis support. Electrolyte imbalance, particularly hyperkalemia, can further complicate the clinical course. Although most survivors eventually recover renal function, recovery may take several weeks or months depending on disease severity.
Pulmonary Involvement: Pulmonary complications are the defining feature of HPS. Increased vascular permeability in pulmonary capillaries causes rapid leakage of fluid into alveolar spaces, resulting in noncardiogenic pulmonary edema. Patients typically develop progressive cough, dyspnea, hypoxia, and respiratory distress that may rapidly advance to acute respiratory failure. Mechanical ventilation is often required in severe cases.
Cardiac Involvement: Cardiac involvement may occur in severe hantavirus infection and contributes significantly to morbidity and mortality. Myocardial depression, reduced cardiac output, and circulatory dysfunction may lead to hypotension and cardiogenic shock, particularly in advanced HPS.
Signs and symptoms of Hantavirus infection
Clinical manifestations of hantavirus infection vary depending on the viral species and disease syndrome.
Hemorrhagic fever with renal syndrome (HFRS)
HFRS generally progresses through five clinical phases:
1. Febrile Phase
This phase lasts 3-7 days and is characterized by:
- Sudden onset of high fever
- Chills
- Headache
- Myalgia (muscle pain or aches)
- Back pain
- Abdominal pain
- Nausea and vomiting
- Facial flushing
- Conjunctival injection
2. Hypotensive phase
Capillary leakage leads to hypotension and shock. Patients may develop tachycardia (increased heart rate) and circulatory collapse.
3. Oliguric (renal dysfunction) phase
Renal dysfunction becoymes prominent with:
- Reduced urine output
- Proteinuria
- Hematuria
- Elevated serum creatinine
- Hyperkalemia
Severe cases may progress to acute kidney injury.
4. Diuretic phase
Urine output increases markedly, sometimes reaching several liters per day. Electrolyte imbalance and dehydration may occur.
5. Convalescent phase
Recovery may take weeks to months. Renal function gradually improves.
Hantavirus pulmonary syndrome (HPS)
HPS progresses rapidly and often has a mortality rate of 30-40%. The phases involved are:
1. Prodromal phase
Initial symptoms for this phase resemble influenza-like illness:
- Fever
- Fatigue
- Myalgia
- Headache
- Dizziness
- Gastrointestinal symptoms
2. Cardiopulmonary phase
During this phase, patients develop severe respiratory compromise within days. The signs include:
- Cough
- Shortness of breath
- Tachypnea (rapid slow breathing)
- Hypoxia (lack of oxygen at the tissue level)
- Pulmonary edema
- Hypotension
- Shock
Respiratory failure may require mechanical ventilation.
3. Convalescent phase: Survivors gradually recover over weeks or months.
Laboratory detection and diagnosis of Hantavirus infection
Accurate laboratory diagnosis of Hantavirus infection is essential because clinical manifestations may resemble influenza, leptospirosis, dengue fever, malaria, or other viral hemorrhagic fevers.
Specimen collection
Common clinical specimens include:
- Blood
- Serum
- Plasma
- Tissue samples
- Respiratory specimens
Biosafety precautions are important because hantaviruses are potentially hazardous pathogens.
Serological methods
Serology is the primary diagnostic approach for Hantavirus infection; and these serological methods are:
- Enzyme-Linked Immunosorbent Assay (ELISA): ELISA is widely used because it is sensitive and relatively simple. It detects hantavirus-specific IgM and IgG antibodies. IgM antibodies indicate recent infection. Rising IgG titers confirm infection.
- Immunofluorescence Assay (IFA): IFA can detect antibodies against hantavirus antigens using fluorescent labeling.
- Immunoblotting: Western blot assays help confirm serological findings.
Molecular Methods
- Reverse Transcription Polymerase Chain Reaction (RT-PCR): RT-PCR detects viral RNA during acute infection and allows identification of specific hantavirus species. This method is highly sensitive and useful for early diagnosis.
- Real-Time PCR: Real-time PCR provides quantitative detection and rapid turnaround time.
- Sequencing: Genome sequencing supports epidemiological studies, outbreak investigations, and phylogenetic analysis.
Virus isolation: Virus isolation is possible in cell culture but is technically demanding and requires high-level biosafety laboratories.
Histopathology
Tissue examination for detecting Hantavirus infection may reveal:
- Interstitial edema
- Hemorrhage
- Mononuclear infiltration
- Acute tubular necrosis
- Pulmonary edema
Immunohistochemistry can demonstrate viral antigens in tissues.
Treatment of Hantavirus infection
Currently, there is no universally approved specific antiviral therapy for hantavirus infection, and therefore management is primarily based on early diagnosis, intensive supportive care, and prompt stabilization of vital organ functions, which are critical for improving patient survival and reducing complications. In patients with HFRS or HPS, careful clinical monitoring is essential because the disease can progress rapidly to respiratory failure, shock, or acute kidney injury. One of the most important aspects of treatment is careful fluid management, since excessive intravenous fluid administration may worsen pulmonary edema due to increased vascular permeability, while insufficient fluid replacement can aggravate hypotension and circulatory shock.
Patients who develop respiratory distress or hypoxia require immediate oxygen therapy, and severe HPS cases often need mechanical ventilation to maintain adequate oxygenation during acute respiratory failure. In addition, patients with severe hypotension may require hemodynamic support using vasopressors to maintain blood pressure and organ perfusion. In severe HFRS cases complicated by acute kidney injury, dialysis or renal replacement therapy may be necessary until renal function gradually recovers during convalescence.
Antiviral therapy for hantavirus infection remains limited, although Ribavirin has demonstrated some effectiveness against HFRS when administered during the early stages of infection. Studies suggest that the drug may reduce disease severity and mortality in selected patients; however, its clinical benefit in HPS remains uncertain because available evidence is limited and inconsistent. In addition, the widespread use of Ribavirin is constrained by potential adverse effects and variable therapeutic outcomes.
In critically ill patients with severe HPS complicated by refractory respiratory failure or cardiogenic shock, extracorporeal membrane oxygenation (ECMO) has emerged as an important supportive intervention that may significantly improve survival by maintaining adequate oxygenation and circulatory support while the lungs and heart recover. Ongoing research efforts are focused on the development of novel therapeutic and preventive strategies, including the use of monoclonal antibodies, convalescent plasma therapy, new antiviral compounds, immune modulators, and vaccine development. Several experimental vaccines and immunotherapeutic approaches have shown encouraging results in animal models and early-phase clinical trials, offering hope for improved prevention and treatment of hantavirus infections in the future.
Prevention and control of Hantavirus infection
Because no widely available vaccine exists for general human use in the face of a potential Hantavirus infection, prevention focuses on reducing human exposure to infected rodents. Some of the important preventive measures adopted are as follows:
- Rodent control: Rodent population management is essential to prevent Hantavirus infection particularly in endemic areas or regions. Some of the important measures usually taken to control rodent infestation include: eliminating food sources, sealing entry points in buildings, proper waste disposal, trapping rodents, and maintaining clean surroundings.
- Environmental Hygiene: Areas contaminated with rodent excreta should be cleaned carefully. Some important recommended precautions include: wearing gloves and masks, ventilating enclosed spaces before cleaning, avoiding sweeping or vacuuming dry droppings, and using disinfectants such as bleach solutions.
- Occupational safety: Individuals who are at higher risk of Hantavirus infection include: farmers, forestry workers, military personnel, laboratory workers, and construction workers – who may be exposed to aerosolized particles of Hantavirus. Protective equipment and education reduce occupational exposure.
- Public health education: Awareness campaigns is important to control and prevent Hantavirus infection because it will help communities to understand: the modes of transmission of the virus, safe cleaning practices to prevent it, rodent-proofing techniques, and possible early recognition of symptoms.
Epidemiology of Hantavirus
Hantavirus infections occur worldwide, and their geographic distribution is largely determined by the presence and ecology of specific rodent reservoir hosts that maintain the virus in nature. Globally, the epidemiology of hantavirus disease varies considerably across regions, with different viral species causing distinct clinical syndromes. Asia carries the highest burden of HFRS, with China reporting the majority of global HFRS cases annually, primarily associated with Hantaan virus and Seoul virus, while countries such as South Korea and Russia also experience substantial disease incidence and periodic outbreaks.
In Europe, the most prevalent hantavirus is Puumala virus, which is widely distributed across Northern and Central European countries including Finland, Sweden, Germany, Belgium, and France. European hantavirus infections are generally milder than the severe forms of HFRS commonly observed in Asia, although significant morbidity still occurs. In the Americas, hantavirus infections are mainly associated with HPS, a severe respiratory disease with high mortality rates.
The United States reports sporadic cases, particularly in western regions where deer mice are abundant and serve as the principal reservoir ofSin Nombre virus. In addition, severalSouth American countries such as Argentina, Chile, Brazil, and Panama have documented outbreaks caused byAndes virus and related hantaviruses, with some strains demonstrating limited person-to-person transmission.
Reservoir ecology of Hantavirus
Rodent population density strongly influences hantavirus transmission. Some of the most important environmental factors affecting rodent abundance include:
- Rainfall
- Temperature
- Food availability
- Deforestation
- Agricultural expansion
- Climate variability
Increased rainfall can enhance vegetation growth, leading to population surges in rodents and increased risk of human exposure.
Risk factors for Hantavirus infection
Risk factors for infection with Hantavirus include:
- Living in rodent-infested areas
- Agricultural activities
- Camping or hiking
- Cleaning abandoned buildings (without proper protection)
- Occupational exposure
- Poor sanitation
Outbreaks of Hantavirus infection
Outbreaks of Hantavirus infection often follow ecological disturbances that increase rodent-human interaction.
Examples include:
- Korean War HFRS outbreak
- 1993 Four Corners outbreak in the United States
- Andes virus outbreaks in South America
Seasonal variation of Hantavirus infection
Seasonal patterns vary by region.
- HFRS often peaks in autumn and winter.
- HPS incidence may increase during spring and summer when outdoor activities are common.
Climate change and emerging risks to Hantavirus infection spread
Climate change and emerging environmental risks are increasingly recognized as important factors influencing the spread and transmission dynamics of hantavirus infections worldwide. Changes in global temperature, rainfall patterns, humidity, and seasonal variability can significantly affect rodent population density, breeding cycles, migration patterns, and geographic distribution, thereby increasing the likelihood of human exposure to infected reservoir hosts. For example, periods of heavy rainfall may enhance vegetation growth and food availability, leading to rapid increases in rodent populations and a subsequent rise in hantavirus transmission risk.
Global warming on the other hand may expand the habitats of rodent reservoirs into previously non-endemic regions, potentially introducing hantavirus infections into new human populations. Urbanization, deforestation, agricultural expansion, mining activities, and environmental degradation disrupt natural ecosystems and increase human contact with wildlife reservoirs, thereby creating more opportunities for zoonotic spillover events. Increased international travel and human migration may also contribute to the wider dissemination of hantavirus infections, emphasizing the need for enhanced surveillance, environmental monitoring, and integrated One Health approaches to disease prevention and control.
Surveillance for Hantavirus infection outbreak
Integrated surveillance involving human, animal, and environmental health reflects the One Health approach to zoonotic disease control. Effective surveillance systems for early detection of Hantavirus infection are essential for:
- Early outbreak detection
- Monitoring rodent populations
- Identifying emerging strains
- Public health preparedness
References
Mir, M. A. (2010). Hantaviruses. Clinical Laboratory Medicine, 30(1), 67–91.
Easterbrook, J. D., & Klein, S. L. (2008). Immunological mechanisms mediating hantavirus persistence in rodent reservoirs. PLoS Pathogens, 4, e1000172.
Johnson, K. M. (2001). Hantaviruses: History and overview. Current Topics in Microbiology and Immunology, 256, 1–14.
Khaiboullina, S. F., Morzunov, S. P., & St Jeor, S. C. (2005). Hantaviruses: Molecular biology, evolution and pathogenesis. Current Molecular Medicine, 5(8), 773–790.
Khan, A., & Khan, A. S. (2003). Hantaviruses: A tale of two hemispheres. Panminerva Medica, 45(1), 43–51.
Avšič-Županc, T., Saksida, A., & Korva, M. (2019). Hantavirus infections. Clinical Microbiology and Infection, 21(Suppl), e6–e16.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.