
Infectious diseases remain a major cause of morbidity and mortality worldwide despite significant advances in medicine, public health, and disease prevention. The development of an infection is a complex biological process that depends on successful interactions between a pathogenic microorganism and a susceptible host. For an infectious agent to establish itself within the body, it must overcome a series of physical, chemical, and immunological barriers designed to prevent microbial invasion. The ability of pathogens to breach these defenses and gain access to host tissues represents a critical step in the chain of infection and often determines whether exposure will result in colonization, disease, or elimination of the microorganism.
The human body is continuously exposed to a vast array of microorganisms present in the environment, including bacteria, viruses, fungi, and parasites. While many of these microorganisms are harmless or even beneficial, some possess the capacity to cause disease when favorable conditions arise. Exposure to a pathogen alone does not necessarily lead to infection. Successful infection depends on several factors, including the virulence of the microorganism, the size of the infectious dose, environmental conditions, and the host’s immune status. A fundamental requirement, however, is that the pathogen must first gain access to the internal environment of the host where it can survive, multiply, and evade defensive mechanisms.
The body possesses multiple layers of protection that serve as the first line of defense against microbial invasion. Intact skin acts as a highly effective physical barrier, while mucosal surfaces produce secretions containing antimicrobial substances that inhibit pathogen growth. Additional protective mechanisms such as normal microbiota, acidic environments, mucus production, and immune surveillance collectively reduce the likelihood of infection. Nevertheless, many infectious agents have evolved specialized adaptations that enable them to circumvent or overcome these protective barriers. Through evolutionary processes, pathogens have developed mechanisms that facilitate attachment to host tissues, resistance to antimicrobial substances, invasion of cells, and evasion of immune responses.
An understanding of how infectious agents gain access to the body is essential for comprehending disease transmission and pathogenesis. The initial interaction between a pathogen and its host often determines the subsequent course of infection, influencing the site of disease, severity of clinical manifestations, and potential for further transmission. The point at which a microorganism first enters a susceptible host serves as a crucial stage in the infectious process because it provides the opportunity for the pathogen to establish itself and initiate disease-producing activities. Consequently, knowledge of pathogen entry is fundamental to epidemiology, infection prevention, and public health interventions.
The study of pathogen entry also has important implications for disease control strategies. Many preventive measures, including vaccination programs, personal protective practices, sanitation measures, and infection-control protocols, are designed to interrupt the earliest stages of microbial invasion. By understanding the mechanisms through which infectious agents access the body, healthcare professionals and public health practitioners can develop targeted approaches to reduce exposure, limit transmission, and protect vulnerable populations. Therefore, an appreciation of the pathways and mechanisms involved in the entry of infectious agents provides an essential foundation for understanding infectious disease dynamics and the measures required to prevent their occurrence and spread.
Pathogenic microorganisms enter the human body through various routes or portals of entry, which serve as pathways by which infectious agents such as bacteria, viruses, fungi, and protozoa penetrate host defense barriers and establish infection. These routes are diverse and reflect the wide range of environmental exposures and transmission mechanisms involved in infectious disease spread. The specific route of entry often influences the site of initial infection as well as the progression and severity of disease, since different pathogens are adapted to exploit particular anatomical and physiological pathways.
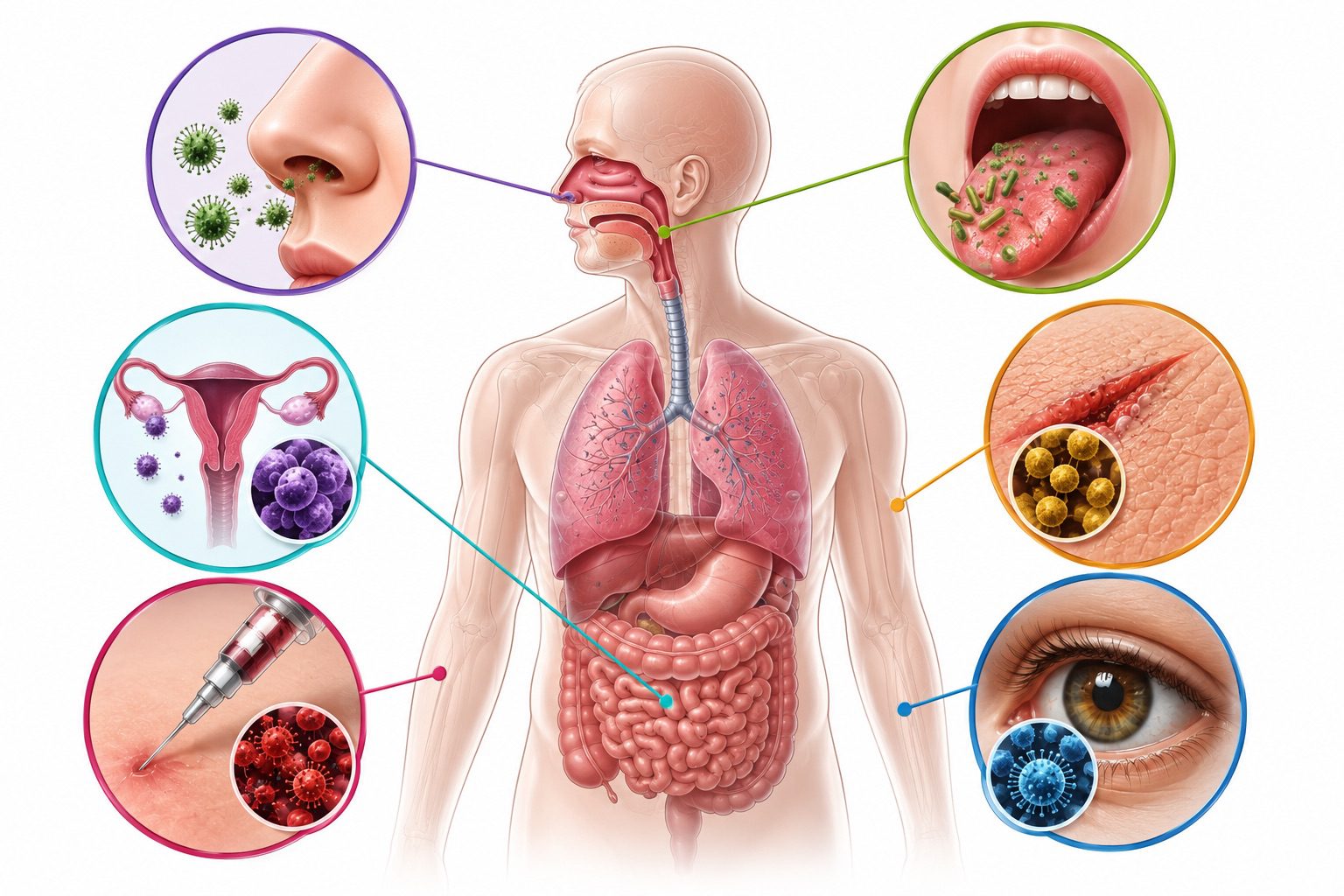
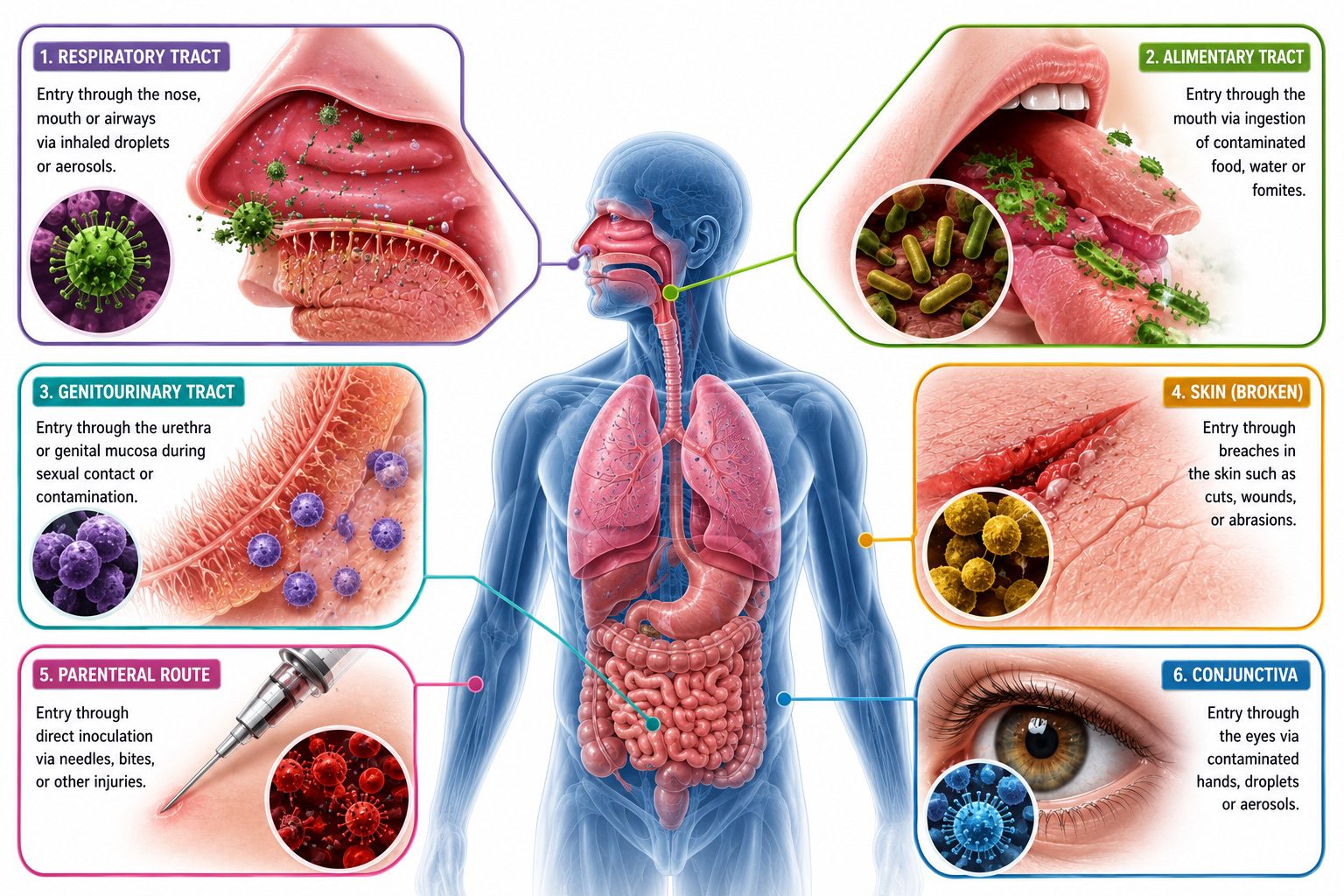
The main portals of entry of infectious agents into the human body include the respiratory tract, the gastrointestinal tract, the genitourinary tract, the skin and subcutaneous tissues, the conjunctiva and other mucous membranes, the bloodstream through parenteral routes, the placenta (transplacental transmission), entry through animal or insect bites and other vector-mediated mechanisms, and direct inoculation through breaks in the skin such as cuts, wounds, burns, or surgical interventions.
These routes of pathogenic entry into the human body collectively represent the primary means by which infectious agents gain access to internal tissues (Figure 1). Although the human body possesses multiple structural and immunological defenses designed to prevent invasion, pathogens may still enter when these barriers are compromised or when microorganisms possess specific virulence factors that enable attachment, penetration, or immune evasion.
The skin as a portal of entry for infectious agents
The skin is the largest organ of the human body and serves as the first line of defense against the invasion of pathogenic microorganisms. Under normal conditions, intact skin acts as an effective physical and biological barrier that prevents bacteria, viruses, fungi, and parasites from gaining access to underlying tissues and the bloodstream. Its protective function is enhanced by several factors, including the continuous shedding of dead skin cells, the presence of normal microbiota, the production of antimicrobial substances, and the relatively dry and acidic environment of the skin surface. Together, these characteristics make healthy skin highly resistant to microbial colonization and infection.
Despite its remarkable protective capacity, the skin can become a portal of entry for infectious agents when its integrity is compromised. Any disruption of the skin surface, such as cuts, abrasions, puncture wounds, surgical incisions, burns, ulcers, or other forms of trauma, creates an opportunity for microorganisms to bypass the body’s natural defenses and invade deeper tissues. Once these pathogens penetrate the skin barrier, they may multiply locally, spread through surrounding tissues, or enter the bloodstream and lymphatic system, leading to localized or systemic infections. The severity of the resulting infection often depends on the virulence of the invading microorganism, the extent of tissue damage, and the immune status of the affected individual.
Animal bites and arthropod bites also represent important means through which infectious agents gain entry into the human body. During biting or feeding activities, microorganisms may be directly introduced into the skin and underlying tissues. Numerous infectious diseases are transmitted in this manner, with insects and other arthropods acting as vectors that carry pathogens from one host to another. Similarly, bites from infected animals can introduce disease-causing microorganisms through the puncture wounds they create. These routes of entry bypass many of the protective mechanisms associated with intact skin and facilitate the establishment of infection.
The skin’s natural resistance to microbial growth is partly attributable to its relatively dry surface. Most pathogenic microorganisms require moisture and suitable nutrients for growth and multiplication; therefore, the dry nature of healthy skin inhibits the survival and proliferation of many pathogens. In addition, sweat and sebaceous secretions contain antimicrobial compounds that further limit microbial colonization. The normal microbial flora of the skin also contributes to protection by competing with potentially harmful microorganisms for nutrients and space, thereby reducing the likelihood of pathogen establishment.
Nevertheless, certain microorganisms can thrive under specific conditions on the skin. For example, excessive secretion of sebum, an oily substance produced by sebaceous glands, can create a favorable environment for the growth of some bacteria. One notable example is Cutibacterium acnes (formerly Propionibacterium acnes), a Gram-positive bacterium commonly associated with acne. The proliferation of this organism within blocked hair follicles and sebaceous glands triggers inflammatory responses that result in the formation of pimples, blackheads, and other acne lesions. Although acne is generally not considered a severe infectious disease, it illustrates how alterations in the skin environment can promote microbial growth and contribute to disease development. The skin serves as a highly effective barrier against infection; however, whenever its protective integrity is breached or its normal physiological conditions are altered, it can become an important portal through which infectious agents enter the body and initiate disease.
The gastrointestinal tract as a portal of entry for infectious agents
The gastrointestinal tract (GIT), also known as the alimentary canal, is a complex organ system primarily responsible for the ingestion, digestion, absorption, and utilization of nutrients necessary for growth, energy production, and the maintenance of normal physiological functions. Extending from the mouth to the anus, the gastrointestinal tract serves as a critical interface between the external environment and the internal tissues of the body. While its principal role is to facilitate nutrition and maintain homeostasis, it also represents a significant route through which infectious agents can gain access to the human body.
Every day, humans consume food and water that may contain a wide variety of microorganisms. Although the gastrointestinal tract possesses several protective mechanisms, including gastric acidity, digestive enzymes, mucus secretion, normal intestinal microbiota, and immune defenses, these barriers are not always sufficient to prevent infection. Numerous pathogenic microorganisms have evolved strategies that enable them to survive the harsh conditions of the digestive system, colonize the intestinal tract, and cause disease. Consequently, the ingestion of contaminated food, water, or other substances constitutes one of the most common modes of transmission for many infectious diseases worldwide.
Pathogens enter the body through the gastrointestinal tract primarily through the mouth following the consumption of food or beverages contaminated with infectious microorganisms or their toxins. These contaminants may include bacteria, viruses, protozoa, and other disease-causing agents capable of surviving transit through the digestive system. Once ingested, some pathogens remain confined to the intestinal tract where they cause localized infections, while others penetrate the intestinal mucosa and disseminate to distant organs and tissues through the bloodstream or lymphatic system. The severity of infection depends on factors such as the type of pathogen, the infectious dose, the virulence characteristics of the microorganism, and the immune status of the host.
Food contamination can occur at multiple stages along the food production and supply chain, including cultivation, harvesting, processing, transportation, storage, preparation, and serving. Poor hygiene practices during food handling and processing provide opportunities for pathogenic microorganisms to contaminate food products directly. Inadequate handwashing, the use of contaminated water, improper storage temperatures, cross-contamination between raw and cooked foods, and unsanitary processing environments are among the major factors that contribute to foodborne infections. In addition to direct contamination, some microorganisms produce toxins in food before consumption. These toxins may remain biologically active even when the microorganisms themselves are no longer viable, resulting in illness following ingestion.
Foodborne and waterborne diseases remain important public health concerns globally, particularly in regions where sanitation infrastructure, food safety systems, and access to clean water are inadequate. Outbreaks associated with contaminated food and water can affect large populations and impose substantial health and economic burdens on communities. Therefore, understanding the gastrointestinal tract as a portal of entry for infectious agents is essential for appreciating the epidemiology of many infectious diseases. This knowledge also underpins the development of effective preventive measures, including proper food hygiene, safe water practices, adequate sanitation, public health education, and food safety regulations aimed at reducing the risk of infection and protecting human health.
The respiratory tract as a major portal of entry for infectious agents
The respiratory tract is one of the most important and frequently utilized portals of entry for infectious agents into the human body. Owing to its continuous exposure to the external environment and the large volume of air inhaled daily, the respiratory system provides numerous opportunities for microorganisms to come into contact with susceptible host tissues. As humans breathe, airborne particles, droplets, and aerosols containing microorganisms may be inhaled into the upper or lower respiratory tract, making this route a highly efficient pathway for the transmission and establishment of infectious diseases.
Many human pathogens, including bacteria, viruses, and fungi, exploit the respiratory tract as their primary means of entry. Among these groups, fungi are particularly dependent on this route because most pathogenic fungal species produce spores or conidia that become dispersed in the atmosphere. These microscopic reproductive structures are widely distributed in air, soil, dust, decaying organic matter, and other environmental reservoirs. When inhaled by susceptible individuals, fungal spores can reach the respiratory passages and, under favorable conditions, germinate and initiate infection. Examples of fungal pathogens that commonly enter the body through inhalation include species of Aspergillus, Histoplasma, Blastomyces, and Coccidioides. The respiratory route therefore plays a central role in the epidemiology of many fungal diseases.
Numerous bacterial pathogens also gain access to the body through the respiratory tract. Organisms such as Mycobacterium tuberculosis, Corynebacterium diphtheriae, Bordetella pertussis, and Haemophilus influenzae are transmitted primarily through inhalation of infectious particles released from infected individuals. Likewise, many viral pathogens, including influenza viruses, respiratory syncytial virus (RSV), adenoviruses, coronaviruses, and rhinoviruses, utilize the respiratory tract as their principal portal of entry. Once inhaled, these microorganisms may colonize the respiratory mucosa, multiply within host tissues, and subsequently cause localized or systemic disease.
Infections transmitted through the respiratory tract are commonly referred to as respiratory or droplet-borne infections because transmission frequently occurs through respiratory droplets and aerosols generated during coughing, sneezing, talking, laughing, or even breathing. These droplets may contain large numbers of viable microorganisms capable of infecting susceptible individuals who inhale them or who come into contact with contaminated respiratory secretions. The risk of transmission is often increased in crowded environments, poorly ventilated spaces, healthcare settings, schools, and other locations where close interpersonal contact facilitates the spread of infectious particles.
Although the respiratory tract possesses several protective mechanisms, including nasal hairs, mucus production, ciliary action, cough reflexes, and immune defenses, many pathogens have evolved strategies to overcome these barriers. Some microorganisms possess specialized surface structures that facilitate attachment to respiratory epithelial cells, while others produce toxins or virulence factors that damage host tissues and promote invasion. Certain pathogens can even evade immune responses, allowing them to persist within the respiratory system and establish infection.
Because of its accessibility, extensive surface area, and constant interaction with the external environment, the respiratory tract remains one of the most significant portals of entry for infectious agents. Understanding the role of the respiratory system in disease transmission is essential for developing effective preventive measures, including respiratory hygiene, vaccination, environmental sanitation, adequate ventilation, and the use of personal protective equipment to reduce the spread of infectious diseases.
The genital tract as a portal of entry for infectious agents
The genital tract constitutes one of the most important routes through which infectious agents gain access to the human body. It is a mucosal-lined system that, while equipped with natural defense mechanisms, remains particularly vulnerable to microbial invasion due to its direct exposure to external environments during sexual activity and certain physiological processes such as childbirth. The epidemiological significance of this route is underscored by the global burden of sexually transmitted infections (STIs), which continue to represent a major public health challenge across all age groups, particularly among sexually active populations with limited access to preventive healthcare services.
A wide range of sexually transmitted diseases are acquired through contact with infected bodily fluids, mucosal secretions, or lesions during sexual intercourse. Common examples include gonorrhea, genital herpes, syphilis, genital warts caused by human papillomavirus (HPV), and non-specific urethritis. Transmission typically occurs when individuals engage in unprotected sexual contact with an infected partner, allowing pathogens to be transferred directly to the mucosal surfaces of the genital tract. The moist, warm environment of the reproductive tract provides favorable conditions for microbial survival and replication, particularly when micro-abrasions or epithelial disruptions are present, which may not always be clinically visible.
The susceptibility of the genital tract to infection is influenced by both biological and behavioral factors. From a biological perspective, the mucosal epithelium, although protective, is thinner and more permeable than keratinized skin, making it easier for pathogens to penetrate. Additionally, the presence of mucous secretions and fluctuating hormonal environments may affect local immune defenses. From a behavioral standpoint, practices such as multiple sexual partnerships, inconsistent condom use, and early sexual debut significantly increase exposure risk. Coexisting infections and immunosuppression further enhance vulnerability to acquisition and progression of sexually transmitted pathogens.
In addition to horizontal transmission through sexual contact, infections may also be acquired vertically through the genital tract during childbirth. This occurs when a newborn is exposed to infectious agents present in the maternal genital tract as it passes through the birth canal. Such vertical transmission can result in significant neonatal morbidity and mortality. Conditions associated with this mode of acquisition include neonatal syphilis, neonatal pneumonia, neonatal sepsis, neonatal meningitis, and neonatal ophthalmia. These infections may arise from a variety of pathogens, including bacteria, viruses, and spirochetes, depending on the maternal infection status at the time of delivery.
The consequences of infections acquired through the genital tract extend beyond immediate clinical manifestations. Many sexually transmitted infections may remain asymptomatic for extended periods, facilitating continued transmission and increasing the risk of long-term complications such as infertility, chronic pelvic inflammatory disease, ectopic pregnancy, and certain malignancies, particularly those associated with oncogenic strains of HPV. Furthermore, the social stigma associated with sexually transmitted infections often delays diagnosis and treatment, thereby exacerbating transmission dynamics within communities.
Although less frequently emphasized, the urinary tract may also serve as a pathway for microbial entry under certain conditions, particularly when normal anatomical and physiological barriers are compromised. Ascending infections originating from periurethral contamination can lead to urinary tract infections, especially in females due to their shorter urethral anatomy. This highlights the interconnected nature of the urogenital system in the pathogenesis of infectious diseases.
The genital tract remains a critical and complex portal of entry for infectious agents, shaped by anatomical susceptibility, behavioral practices, and microbial adaptability. Understanding the role of the genital tract in disease transmission is essential for the development of effective preventive strategies, including safe sexual practices, screening programs, maternal health interventions, and public health education aimed at reducing the burden of sexually transmitted and perinatally acquired infections.
Entry of pathogens through blood transfusion
Blood transfusion is a critical medical procedure involving the intravenous administration of blood or blood components collected from a healthy donor into a recipient. It is primarily performed to restore blood volume, improve oxygen-carrying capacity, or replace deficient blood components in patients suffering from conditions such as severe haemorrhage, anaemia, trauma, surgical blood loss, or hematological disorders. By directly supplying functional red blood cells, plasma, platelets, or clotting factors, transfusion therapy can be life-saving and is a cornerstone of modern clinical medicine.
Despite its therapeutic value, blood transfusion also represents a potential route for the transmission of infectious agents when appropriate safety measures are not strictly observed. Because the procedure involves direct introduction of biological material into the bloodstream, any contaminating pathogen present in donated blood gains immediate access to the recipient’s internal environment, bypassing many of the body’s natural protective barriers. This makes transfusion-transmitted infections particularly efficient and potentially severe, as pathogens are delivered directly into circulation where they can rapidly disseminate to target organs and tissues.
The safety of blood transfusion depends heavily on rigorous donor selection, laboratory screening, and proper handling of blood products. Screening is designed to detect known infectious agents in donated blood before it is released for clinical use. However, when screening is inadequate, improperly conducted, or unable to detect infections during their early stages, contaminated blood may be inadvertently transfused into patients. In such cases, the recipient is exposed to a range of blood-borne pathogens, including viruses, bacteria, and parasites, some of which may cause chronic, life-threatening disease.
Among the most clinically significant transfusion-transmitted infections are those caused by viruses such as the Human Immunodeficiency Virus (HIV), responsible for Acquired Immunodeficiency Syndrome (AIDS), and hepatitis viruses, particularly Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV). These pathogens are of major public health concern because they can establish long-term infection, leading to progressive organ damage, immune dysfunction, or liver failure. In addition to viral agents, certain bacterial infections may also be transmitted through contaminated blood, especially when storage conditions are compromised or when aseptic techniques are not properly maintained. Parasitic infections such as malaria have also been documented in regions where screening for parasitic contamination is insufficient.
The risk of transfusion-associated infection is influenced by several factors, including the prevalence of infectious diseases in the donor population, the sensitivity of screening technologies, and adherence to blood safety protocols. Window periods (intervals between initial infection and detectability by laboratory tests) also contribute to residual risk, as infected donors may test negative despite carrying transmissible pathogens. Consequently, continuous improvement in diagnostic methods, stringent regulatory frameworks, and comprehensive donor evaluation remain essential for minimizing these risks.
In modern healthcare systems, blood transfusion services are governed by strict quality control measures intended to ensure maximum safety for recipients. These include serological testing, nucleic acid amplification techniques, donor deferral policies, and proper storage and handling of blood products. Nevertheless, transfusion remains a potential route of infection if any step in this safety chain is compromised. While blood transfusion is an indispensable medical intervention that saves countless lives, it also underscores the importance of vigilance in infection control practices. Ensuring the microbiological safety of donated blood is essential to preventing the transmission of infectious agents and maintaining the integrity of transfusion medicine.
Entry of pathogens through the congenital route
Congenital transmission represents a specialized and clinically significant pathway by which infectious agents are passed from a mother to her developing offspring during pregnancy. Unlike postnatal transmission, which occurs after birth through environmental exposure or interpersonal contact, congenital transmission occurs in utero and involves the direct passage of pathogens across maternal-fetal interfaces. This route of infection is of particular importance because it can result in early fetal exposure during critical stages of development, often leading to severe developmental abnormalities, chronic infection, miscarriage, stillbirth, or neonatal disease.
The process of congenital infection is closely linked to the biological relationship between the maternal and fetal circulatory systems. During pregnancy, the placenta serves as the essential organ of exchange, facilitating the transfer of nutrients, gases, and waste products between mother and fetus. While the placenta provides a highly specialized protective barrier, it is not completely impermeable. Certain microorganisms have evolved mechanisms that allow them to bypass or penetrate placental defenses, gaining access to fetal tissues and establishing infection. Once inside the fetal environment, pathogens may disseminate widely due to the immature immune system of the developing fetus, which is less capable of mounting effective immune responses.
A variety of infectious agents are capable of vertical transmission. Among the most clinically important are viral pathogens such as human immunodeficiency virus (HIV), cytomegalovirus (CMV), rubella virus, and Zika virus. Bacterial agents such as Treponema pallidum, the causative organism of syphilis, and Listeria monocytogenes are also well-documented causes of congenital infections. Additionally, parasitic organisms such as Toxoplasma gondii can cross the placenta and cause significant fetal damage. These infections are often collectively categorized as congenital or intrauterine infections, emphasizing their origin prior to birth.
The timing of maternal infection plays a crucial role in determining fetal outcomes. Early pregnancy infections are more likely to cause structural malformations and organogenesis defects because this is a period of rapid cellular differentiation and organ formation. In contrast, infections acquired later in pregnancy may lead to functional impairments, growth restriction, or systemic illness in the neonate. The severity of congenital disease is therefore influenced not only by the type of pathogen involved but also by the gestational stage at which transmission occurs.
Transmission to the fetus may occur through different mechanisms. In some cases, pathogens cross the placental barrier directly through trophoblastic cells. In others, infection of placental tissues leads to inflammation and disruption of the barrier integrity, facilitating passage into fetal circulation. Once established, the pathogen may replicate within fetal tissues, including the liver, brain, and blood-forming organs, leading to multisystem involvement. The clinical consequences of congenital infections are often severe and may include neurological impairment, congenital anomalies, hepatosplenomegaly, jaundice, and long-term developmental delay.
Preventing congenital infections is a key component of maternal and child health programs. Strategies such as antenatal screening, early diagnosis and treatment of maternal infections, vaccination prior to pregnancy, and education on preventive behaviors significantly reduce the risk of vertical transmission. Infections such as HIV have demonstrated that with appropriate antiretroviral therapy during pregnancy and delivery, the risk of mother-to-child transmission can be dramatically reduced. Congenital transmission is a critical pathway in the epidemiology of infectious diseases, representing a direct interface between maternal infection and fetal vulnerability.
Entry of pathogens through the eyes or conjunctiva
The ocular surface, particularly the conjunctiva, represents a clinically important but often underappreciated route through which infectious agents may gain access to the body. Although the eye is equipped with several protective mechanisms designed to limit microbial colonization and invasion, it remains vulnerable to infection due to its constant exposure to the external environment and frequent contact with potentially contaminated materials. The conjunctiva, a thin, transparent mucous membrane covering the sclera and lining the inner surfaces of the eyelids, provides a moist and vascularized surface that can support the adherence and, in some cases, the establishment of pathogenic microorganisms.
Infectious agents may reach the ocular surface through direct contact with contaminated hands, respiratory droplets, or fomites such as towels, cosmetics, or medical instruments. Indirect transmission is particularly relevant in environments where hygiene practices are inadequate, allowing microorganisms to be transferred from contaminated surfaces to the eye during routine activities such as rubbing the eyes or improper handling of contact lenses. Once deposited on the conjunctival surface, pathogens may exploit microa-brasions or disruptions in the epithelial barrier to initiate localized infection or, in certain cases, extend to deeper ocular structures.
The eye is normally protected by a combination of mechanical, chemical, and immunological defenses. The blinking reflex helps to physically remove foreign particles, while tears provide continuous flushing of the ocular surface. Tear fluid contains antimicrobial substances such as lysozyme, lactoferrin, and immunoglobulin A, which collectively inhibit microbial growth and facilitate pathogen clearance. In addition, the integrity of the conjunctival epithelium acts as a physical barrier that limits microbial penetration. Despite these defenses, certain pathogens have evolved strategies to evade or overcome ocular protective mechanisms, allowing them to persist and multiply on the conjunctival surface.
Neonates are particularly vulnerable to infections involving the conjunctiva due to their immature immune systems and the circumstances surrounding birth. During vaginal delivery, the newborn’s eyes may come into direct contact with maternal genital secretions, which can harbor infectious organisms. This exposure can result in colonization of the conjunctival surface and, if untreated, progression to more severe ocular disease. The risk is further heightened in cases where maternal infections are present, especially those involving sexually transmitted pathogens. The absence of a fully developed adaptive immune response in neonates contributes to the increased susceptibility and potential severity of infection in this population.
Infections acquired through the conjunctiva can range from mild, self-limiting inflammation to severe conditions that threaten vision if not promptly managed. The clinical outcome depends on factors such as the virulence of the infecting organism, the inoculum size, and the host immune response. Early recognition and preventive interventions are therefore essential to reduce the burden of ocular infections. Prophylactic measures, particularly in neonatal care, play a critical role in minimizing transmission during delivery and protecting the developing eye from infectious damage. The conjunctival route of entry underscores the importance of ocular hygiene, infection control practices, and preventive neonatal care in reducing the risk of pathogen transmission.
Entry of pathogens through parenteral routes
Parenteral transmission refers to the entry of infectious agents directly into the body through breaches in the skin or mucosal barriers, bypassing the natural protective mechanisms that ordinarily prevent microbial invasion. Unlike routes that require organisms to traverse intact epithelial surfaces, parenteral entry provides pathogens with immediate access to internal tissues and, in many cases, the bloodstream. This mode of transmission is therefore highly efficient and often associated with rapid systemic dissemination of infection. It is a significant concern in both clinical and community settings because even minute quantities of infectious material can be sufficient to establish disease.
One of the most well-recognized mechanisms of parenteral transmission involves the use of needles and syringes. When medical injections are administered, strict aseptic technique is required to prevent the inadvertent transfer of microorganisms between patients. However, when injection equipment is reused or improperly sterilized, it can become a direct vehicle for pathogen transmission. This risk is particularly pronounced in settings with limited resources or inadequate infection control practices, where sterilization protocols may not be consistently followed. In such circumstances, contaminated injection devices can facilitate the spread of bloodborne pathogens, making parenteral transmission a major public health concern.
Beyond clinical environments, parenteral transmission is also a significant issue among individuals who use injectable drugs. The sharing of needles or syringes introduces a direct pathway for the exchange of blood and bodily fluids between individuals, creating an efficient route for pathogen spread. This behavior has been strongly associated with the transmission of several clinically important infectious agents, most notably human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV). These viruses are particularly well adapted to survival and infectivity in blood, and even microscopic contamination of injection equipment can be sufficient for transmission. The resulting infections often become chronic, leading to long-term health complications such as liver cirrhosis, hepatocellular carcinoma, and progressive immunodeficiency.
In addition to injection-related exposures, parenteral transmission can also occur through other forms of skin penetration. These include accidental needlestick injuries in healthcare settings, contaminated surgical instruments, tattooing and body piercing procedures, and exposure to sharp objects contaminated with infected blood. Healthcare workers are especially at risk due to frequent contact with sharp instruments and blood-containing materials. Consequently, adherence to standard precautions including the use of personal protective equipment, safe handling of sharps, and proper disposal of medical waste is essential in reducing occupational exposure.
Prevention of parenteral transmission relies heavily on strict infection control measures. In medical practice, the use of single-use disposable syringes and needles is strongly recommended, along with proper sterilization of reusable instruments. Safe injection practices, including never reusing syringes between patients and maintaining aseptic technique during all invasive procedures, are fundamental principles of modern healthcare. In community settings, harm reduction strategies such as needle exchange programs and education on safe injection practices have proven effective in reducing the spread of bloodborne infections among people who inject drugs. Parenteral routes represent a highly efficient and clinically important pathway for the transmission of infectious agents. Because this mode of entry bypasses the body’s primary defensive barriers, infections acquired in this manner often have serious consequences.
References
Black, J.G. (2008). Microbiology: Principles and Explorations (7th ed.). Hoboken, NJ: J. Wiley & Sons.
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA.
Champoux J.J, Neidhardt F.C, Drew W.L and Plorde J.J (2004). Sherris Medical Microbiology: An Introduction to Infectious Diseases. 4th edition. McGraw Hill Companies Inc, USA.
Dictionary of Microbiology and Molecular Biology, 3rd Edition. Paul Singleton and Diana Sainsbury. 2006, John Wiley & Sons Ltd. Canada.
Engleberg N.C, DiRita V and Dermody T.S (2007). Schaechter’s Mechanisms of Microbial Disease. 4th ed. Lippincott Williams & Wilkins, Philadelphia, USA.
Gladwin M and Trattler B (2006). Clinical Microbiology Made Ridiculously Simple. 3rd edition. MedMaster, Inc., Miami, USA.
Levinson W (2010). Review of Medical Microbiology and Immunology. Twelfth edition. The McGraw-Hill Companies, USA.
Madigan M.T., Martinko J.M., Dunlap P.V and Clark D.P (2009). Brock Biology of Microorganisms, 12th edition. Pearson Benjamin Cummings Inc, USA. Pp. 902-903.
Mahon C. R, Lehman D.C and Manuselis G (2011). Textbook of Diagnostic Microbiology. Fourth edition. Saunders Publishers, USA.
Mandell G.L, Bennett J.E, Dolin R, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 5th ed. Philadelphia: Churchill Livingstone, 2002.
Murray P.R, Baron E.J, Jorgensen J.H., Pfaller M.A and Yolken R.H (2003). Manual of Clinical Microbiology. 8th edition. Volume 2. American Society of Microbiology (ASM) Press, Washington, D.C, U.S.A.
Murray P.R., Rosenthal K.S., Kobayashi G.S., Pfaller M. A. (2002). Medical Microbiology. 4th edition. Mosby Publishers, Chile.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.

Dr you are doing good God bless you
Hello Ibrahim,
Thank you so much for your kind words.
We are happy that the website was helpful to you and your peers.