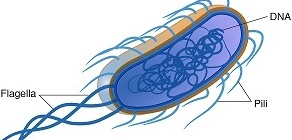
Haemophilus influenza is a small, Gram-negative, non-sporulating, non-motile, urease positive, indole positive, pleomorphic, rod-like or coccobacillus blood-loving bacterium in the family, Pasteurellaceae. H. influenzae, a non-toxin producing bacterium was first isolated during the 1890 influenza pandemic, and it is often referred to as a “blood-loving” bacterium (i.e. haemophilic bacterium) because it requires growth factors which are present in blood for growth. These growth factors are hemin (X factor) and NAD or NADP (V factor), and they play significant role in the growth of H. influenzae.
Haemin is required by H. influenzae to synthesize cytochromes, catalase and peroxidase while nicotinamide adenine dinucleotide (NAD)/nicotinamide adenine dinucleotide phosphate (NADP) is used as an electron carrier by the bacterium in its oxidation-reduction reaction. H. influenzae is a facultative anaerobic bacterium, and it is the only medically important pathogen in the family Pasteurellaceae.The whole chromosome of H. influenzae was successfully sequenced in 1995, making it one of the first free-living bacterium aside Escherichia coli whose entire genome was successfully sequenced.
Thus, H. influenzae is a veritable tool for bacterial transformation and conjugation experiments in the hands of molecular biologists. Other members of bacteria in the Pasteurellaceae family include: Actinobacillus species and Pasteurella species, both of which cause infection in animals. Non-encapsulated strains of H. influenzae is found as normal flora in the mucous membrane of the upper respiratory tract of humans (in particular: the nasopharyngeal region), both children and adults where it occasionally causes upper respiratory tract infections.
Only encapsulated H. influenzae (containing capsular polysaccharides) are known to cause infections in humans, despite the fact that non-encapsulated strains of Haemophilus can also cause infections in children and immunocompromised individuals.Some species in the genus Haemophilus are known pathogens of humans while others are opportunistic and rarely cause infections in humans. In particular, H. influenzae type b (Hib), an encapsulated strain is the chief cause of infections in humans especially children where it causes a variety of infections including bacteraemia, pneumoniae, meningitis, and epiglottis.
In adults, Hib cause cellulitis, emypyema, septic arthritis and other invasive infections. Hib causes the most severe infections in humans. Only a small proportion of humans harbour H. influenzae type b and this strain are primarily responsible for infections in such individuals. Occasionally, non-typable H. influenzae strains (which occur as normal flora in the upper respiratory tract of humans) cause a variety of infections in humans only by chance.
PATHOGENESISOF HAEMOPHILUS INFLUENZAE INFECTION
The respiratory tract is often the major route via which Haemophilus influenzae type b (Hib) enters the body and cause infection. Though the pathogenesis of H. influenzae is not completely explicit, the capsular polysaccharide is believed to be the main driving force behind the microbe’s virulence. The capsular polysaccharide confers protection to H. influenzae from lysis by complement molecules and opsonization by phagocytes. Non-encapsulated strains of H. influenzae rarely cause infections, and it is frequently present in the upper respiratory tract of humans, both adults and children.
Infections with capsulated H. influenzae can occur in children (under the age of 5 years) who lack capsular antibodies which protect the host against Hib infections. Generally, Hib, the capsulated strain of Haemophilus causes the most life-threatening forms of infections in children below the age of 5 years old especially when it becomes invasive, affecting various tissues and causing illnesses that include bacteraemia, cellulitis, osteomyeltis, epiglottitis, arthritis and meningitis. However, Hib rarely cause disease in adult individuals and children above the age of 5 years.
Pneumonia, Otitis media (ear infection), epiglottitis, bacteraemia, and meningitis are some of the infections caused by Hib in infants and children, and these can occasionally be caused by non-typable H. influenzae strains. A breakdown of the host’s immune system allows non-encapsulated H. influenzae strains to cause conjunctivitis and other respiratory infections including bronchitis. In infants and children between six months and 4 years old, H. influenzae is frequently found in the upper respiratory tract due to the low immunity of these individuals. But in adults (with sufficient anti-capsular antibodies), infections with H. influenzae is mostly due to debilitated immune system, superinfections or secondary infections resulting from a primary infection.
LABORATORY DIAGNOSIS OF HAEMOPHILUS INFLUENZAE INFECTION
H. influenzae requires complex nutritional growth requirements for growth (inparticular: blood-containing culture mediathat supplies haemin and NAD/NADP). Sputum, pus, CSF, blood and nasopharyngeal specimens are often the main specimens required for laboratory investigation for H. influenzae infection.Chocolate agar is the best culture media for the growth of H. influenzae in the laboratory, and this agar medium is formed by adding horse blood to a nutrient agar base at a temperature of 80oC.
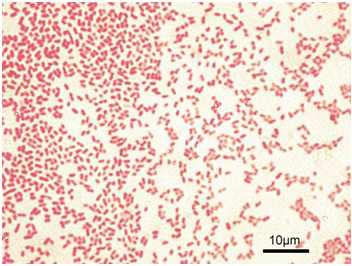
The medium turns chocolate brown in colour, and the warmth nature of the medium releases the X and V factors from the red blood cells (RBCs) of the blood incorporated into the agar base. On horse blood agar, H. influenzae produces small colonies with β-haemolysis. Growth of H. influenzae occurs aerobically with slight CO2 tension (usually 5 %) at 35-37oC. Gram staining of specimens is also very useful when looking out for H. influenzae because smears demonstrate the pleomorphic and thread-like nature of the Gram-negative rods.
Dilute carbol fuchsin instead of safranin (the known and widely used counterstain in Gram staining) is used as the secondary (counter) stain when Gram staining samples suspected to harbour H. influenzae. The demonstration of the requirement for V factor on blood agar is confirmatory for the presence of H. influenzae in a specimen. H. influenzae exhibit satelliting effect on blood agar and this phenomenon demonstrates requirement for V factor.
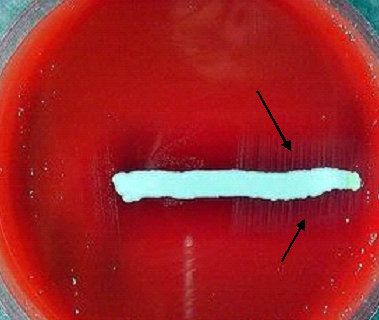
Satellitism (satellite phenomenon) is the observable effect seen when certain growth-factor-requiring microbes (such as H. influenzae) can grow efficiently on a growth media which lacks the required growth factor but which supports the growth of another microorganism which can provide the required growth factor. S. aureus (a feeder organism in this case) is used in performing satellitism test because it supplies V factor into the growth medium, and this phenomenon allows satellite growth of colonies of Haemophilus species that requires NAD/NADP for growth (Figure 1).
H. influenzae does not cause haemolysis on blood agar. Requirement for haemin (X) is investigated by the porphyrin test, and the presence of H. influenzae in the sample is confirmed if the result of the test is negative because H. influenzae does notsynthesize porphyrin and haeme. Only Haemophilus species that do not require X factor for growth are known to be positive for the porphyrin test because such species synthesize haeme and porphyrins. Serological tests can also be employed to detect the serotypes of Haemophilus. H. influenzae is indole and urease positive when subjected to biochemical testing.
IMMUNITY TO HAEMOPHILUS INFLUENZAE INFECTION
Protection against H. influenzae infection in children can be achieved through immunization with Hib conjugate vaccine which elicits bactericidal effect of the host’s phagocytes and complements against the pathogen. Newborns can acquire some level of passive immunity against H. influenzae infections from their mother transplacentally but infection can resurge following the loss of this innate protection which only last for few months after delivery.
Active immunity against Hib infection is developed as the child grows up. The main aspect of the host’s immune resistance against H. influenzae infection is the production of anti-capsular antibodies that support opsonization and lysis of the bacterial pathogen by phagocytes and complements respectively. Immune defense against non-capsulated H. influenzae infections is obtainable in normal adult individuals.
TREATMENT OF HAEMOPHILUS INFLUENZAE INFECTION
The drugs of choice for the treatment of H. influenzae infections include ampicillin, chloramphenicol, sulphamethoxazoles, aminoglycosides, tetracyclines and some third generation cephalosporins including ceftazidime and cefotaxime. Ampicillin is currently rarely used for the treatment of H. influenzae infections due to the production of beta-lactamase enzymes that renders the antibiotic less efficacious.
Augmentin (amoxicillin-clavulanic acid) which impede the production of beta-lactamase enzymes is effective in treating infections caused by non-capsulated H. influenzae strains. Ceftriaxone, a third generation cephalosporin is the best choice for drug in meningitis cases.
Nonetheless, the emergence of plasmid-mediated beta-lactamase enzymes by bacterial pathogens complicates the effectual treatment of H. influenzae infections. Treatment in H. influenzae infection (especially complications involving the central nervous system) should be commenced on time and without delay in order to minimize mortality.
PREVENTION AND CONTROL OF HAEMOPHILUS INFLUENZAE INFECTION
Non-typable species of H. influenzae is a normal flora of the upper respiratory tract of humans. Thus, infections are likely to occur from these species when the immune system becomes weakened. However, Hib can be transmitted from infected persons to non-infected individuals through the respiratory tract as aerosols. Approved Hib conjugate vaccines should be administered to children especially those at higher risk of infection, and booster doses should be included following laid down medical guidelines.
Proper vaccination of children from the age of 2 months and above against the infection will go a long way in minimizing mortality especially bacterial meningitis which is associated with H. influenzae infection. Neisseria meningitidis and Streptococcus pneumoniae are two other bacterial pathogens aside H. influenzae that are the major cause of bacterial meningitis in children globally.
Immunization of adults and children above 60 months of age against H. influenzae infections is however needless because in such individuals, activity immunity against the disease has already been developed. The global usage of Hib conjugate vaccines has helped in reducing the frequency of H. influenzae infections amongst children, and thus has also helped to increase herd immunity against the disease in susceptible populations.
OTHER SPECIES OF HAEMOPHILUS
- Haemophilus ducreyi: H. ducreyi causes chancroid, a sexually transmitted infection (STI) in adults.
- Haemophilus aegyptius: H. aegyptius causes Brazilian purpuric feverin children.
- Haemophilus parainfluenzae: H. parainfluenzae occasionally causes infective endocarditis.
- Haemophilus suis: H. suis causes infection in animals (e.g. pigs).
- Haemophilus aphrophilus: H. aphrophilus occasionally causes pneumonia and endocarditis.
- Haemophilus haemolyticus: H. haemolyticus causes less severe upper respiratory tract infections in children.
References
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA. Pp. 248-260.
Madigan M.T., Martinko J.M., Dunlap P.V and Clark D.P (2009). Brock Biology of microorganisms. 12th edition. Pearson Benjamin Cummings Publishers. USA. Pp.795-796.
Prescott L.M., Harley J.P and Klein D.A (2005). Microbiology. 6th ed. McGraw Hill Publishers, USA. Pp. 296-299.
Ryan K, Ray C.G, Ahmed N, Drew W.L and Plorde J (2010). Sherris Medical Microbiology. Fifth edition. McGraw-Hill Publishers, USA.
Singleton P and Sainsbury D (1995). Dictionary of microbiology and molecular biology, 3rd ed. New York: John Wiley and Sons.
Talaro, Kathleen P (2005). Foundations in Microbiology. 5th edition. McGraw-Hill Companies Inc., New York, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.