Giardiasis is a water-borne protozoal diarrheal-disease that is cause by parasites in the genus Giardia. The disease is a common intestinal infection which is usually spread in human population through feacal-contaminated water, food or hand. Giardiasis was first described by Anthony van Leeuwenhoek in the 1680’s when he examined his stool samples, and discovered tiny moving creatures which he later described as animalcules. The disease is more common in children than in adults, and it has been associated with poor personal hygiene and poor environmental hygiene.
Giardiasisis caused by Giardia species in the genus Giardia. Giardia species include:
- Giardia lamblia (which occur in humans)
- G. muris (which occur in rodents)
- G. agilis
G. lamblia can also be called G. intestinalis or G. duodenalis.
Type and morphology of Giardia species
Giardia species are intestinal flagellates i.e. they are parasites that live in the intestine of their hosts (humans or animals). They can also be called genitourinary flagellates, and they are motile parasites. Giardia species are usually found in the first part of the small intestine (duodenum) and in the jejunum of their host where they carry out their pathogenic and virulent activities. Morphologically, Giardia species (e.g. G. lamblia) exhibits two distinct life forms, and these are the cysts (which is about 10-14 µm long) and the trophozoites (which is heart-shaped and about 10-20 µm long).
The trophozoites (which are the vegetative forms of the parasites) are endowed with four pairs of flagella which help G. lamblia to carryout locomotion and, a sucking (ventral) disk which allows the parasite to attach firmly to the epithelial cells of the host’s intestine. The cysts (which are the infective forms of the parasites) are nonmotile, and they are thick-walled and ellipsoid in shape. Both the cysts and trophozoites are usually recovered from stool samples of infected patients. However, cysts are more common especially in asymptomatic patients of the disease.
Vector, reservoir and habitat of Giardia species
Giardia species has no insect vector. However, the reservoir of the parasite include: humans, rats, dogs, cattle’s and dogs. Giardia parasites are known to live and attaché to the intestinal walls of their hosts.
Clinical signs and symptoms of Giardia infection
The clinical signs and symptoms of Giardiasis include severe diarrhea, body weakness, anorexia, malaise, flatulence (i.e. passing of gas), vomiting, abdominal cramp, growth impairment in children, loss of weight in children and fatigue. In some cases, there are covert carriers of the disease, and such individuals normally harbour large amounts of the parasites cysts in their stool. In addition, the feaces of patients suffering from giardiasis are foul-smelling, profuse and watery; and there is absence of blood since the parasite is not invasive and cannot penetrate vital organs of the body (the spleen, lymph nodes and liver) as is the case for the other protozoan that are flagellates.
Pathogenesis of Giardia infection
The exact virulence and pathogenicity of giardiasis is not well known, but the disease is a watery diarrhea infection that is associated with varying complexities of the parasite coupled with the host’s immune system response to the protozoan. Giardia lamblia (or G. intestinalis) is an intestinal flagellate that parasitizes the intestines of humans causing a range of asymptomatic and symptomatic diarrhea (generally known as giardiasis) which can either be chronic or acute.
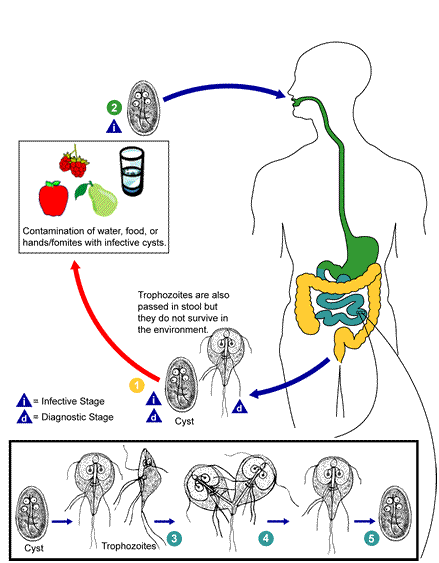
Giardiasis which can either be chronic or acute in terms of its severity starts with the ingestion of Giardia cysts through contaminated water, food or hand (Figure 1). The infection is thus primarily gotten through the feacal-oral route. The human intestine (small and large) is the preferred site of infection for Giardia species. After ingestion of some number of the parasites cysts, the cysts encyst in the first part of the small intestine (i.e. the duodenum), undergo series of multiplication and later transforms to pear-shaped trophozoites (vegetative forms of the parasite).
The trophozoites have sucking disks which allows them to attach to the upper region of the intestinal walls or mucosa and the bowls. Though the Giardia trophozoites attach firmly to the intestinal mucosa of the hosts gastrointestinal tract (GIT), they do not penetrate it as the attachment is merely a key attribute in the virulence and pathogenicity of the parasite to initiate infection and cause the disease. The attachment of the heart- or pear-shaped trophozoites to the intestinal wall of the host adversely affects nutrient absorption by the villi of the intestine. There is also abdominal cramp and consequent chronic or acute watery diarrhea, vomiting and passing of gas (flatulence).
Individuals with suppressed immune system are as liable as children (with poor personal hygiene) in getting the disease than normal adults. The cysts of G. lamblia are very hard and resistant to boiling (when in water or food), and they can survive for several weeks in water. Fomites and dirty hands can also serve as sources via which the parasite reaches the human intestines to initiate an infection. Chronic giardiasis is usually associated with sporadic diarrhea while acute giardiasis produces abdominal pain, anorexia and flatulence in the affected patient.
Laboratory diagnosis of Giardia infection
Protracted and profuse watery diarrhea condition in a patient coupled with some level of loss in weight usually raises clinical suspicion for giardiasis. Feacal examination for parasite’s cysts or egg is usually the first step in the laboratory diagnosis of G. lamblia infection (Figure 2). Concentration techniques are used to demonstrate the parasites ova (egg) while a saline wet mount of fresh watery stool or semi-solid stool samples is used to demonstrate the cysts and trophozoites of the parasite. Trophozoites are usually looked for in watery stool while the cysts of G. lamblia are detected from formed stool samples.
Examination of stool samples for cysts on subsequent days after an initial feacal smear examination is important since G. lamblia cysts formation is not continuous and may be mixed in the first examination. Serological tests that makes use of ELISA techniques that detect the antigen of G. lamblia in stool specimen is also available and used in some cases. Culture and antimicrobial sensitivity testing of G. lamblia are only restricted and performed in research and reference laboratories.
Treatment of Giardia infection
Giardiasis in some cases is asymptomatic (e.g. in children), thus treatment is recommended only for overt individuals (i.e. patients that show obvious clinical signs of the disease). Prompt and appropriate treatment of giardiasis is usually the first step in the effective management of G. lamblia infection. Some of the drugs used for the treatment of G. lamblia infection include metronidazole, furazolidone, tinidazole, quinacrine and paramomycin. Other management therapeutic measures used in giardiasis treatment include maintenance of a good diet and replacement of water loss from the body through oral rehydration. Treatment of asymptomatic individuals of the disease (especially children under the age of 5 who are commonly predisposed to the disease) should be taken with caution, and only administered when necessary.

Control and prevention of Giardia infection
Giardiasis is a disease of poor environmental sanitation and personal hygiene. The parasite that causes the disease (G. lamblia) is usually transmitted via feacally- contaminated water, food or hand. That is, Infection with G. lamblia is through the feacal-oral route. Person-to-person transmission of the infection is possible because G. lamblia cysts continue to remain infectious when passed in the stool of already infected individuals or shortly afterward. Ingestion of G. lamblia cysts through any of these routes allows the parasite to gain entry to the host’s intestines where it disrupts nutrient absorption and cause the disease.
Improvement in personal hygiene, water supplies, food management and environmental sanitation are required to reduce the spread and transmission of the disease. Food and water should be hygienically handled in order to avoid any contact with feaces. Water from the streams and rivers should be properly treated (by boiling, filtration and chlorination) before usage, and feaces should be properly disposed in order to keep water-borne parasites (such as G. lamblia) at bay.
Bore holes, wells, and other water sources should not be dug close to septic tanks and other sewage collection points in order to avoid the infiltration of feacal water into the water sources. Communities should be provided with good and sustainable toilets in order to prevent defeacating in the river and other water ways. Also, sewage and other industrial and domestic wastes should not be disposed into water ways.
References
Aschengrau A and Seage G.R (2013). Essentials of Epidemiology in Public Health. Third edition. Jones and Bartleh Learning,
Beers M.H., Porter R.S., Jones T.V., Kaplan J.L and Berkwits M (2006). The Merck Manual of Diagnosis and Therapy. Eighteenth edition. Merck & Co., Inc, USA.
Chiodini P.L., Moody A.H., Manser D.W (2001). Atlas of medical helminthology and protozoology. 4th ed. Edinburgh: Churchill Livingstone.
Dictionary of Microbiology and Molecular Biology, 3rd Edition. Paul Singleton and Diana Sainsbury. 2006, John Wiley & Sons Ltd. Canada.
Ghosh S (2013). Paniker’s Textbook of Medical Parasitology. Seventh edition. Jaypee Brothers Medical Publishers,
Gillespie S.H and Pearson R.D (2001). Principles and Practice of Clinical Parasitology. John Wiley and Sons Ltd. West Sussex, England.
Gordis L (2013). Epidemiology. Fifth edition. Saunders Publishers, USA.
John D and Petri W.A Jr (2013). Markell and Voge’s Medical Parasitology. Ninth edition.
Kumar V, Abbas A.K, Fausto N and Aster A (2009). Robbins and Cotran Pathologic Basis of Disease. 8th edition. W.B. Saunders Co, USA.
Lee JW (2005). Public health is a social issue. Lancet. 365:1005-6.
Leventhal R and Cheadle R.F (2013). Medical Parasitology. Fifth edition. F.A. Davis Publishers,
Lucas A.O and Gilles H.M (2003). Short Textbook of Public Health Medicine for the tropics. Fourth edition. Hodder Arnold Publication, UK.
MacMahon B., Trichopoulos D (1996). Epidemiology Principles and Methods. 2nd ed. Boston, MA: Little, Brown and Company. USA.
Mandell G.L., Bennett J.E and Dolin R (2000). Principles and practice of infectious diseases, 5th edition. New York: Churchill Livingstone.
Molyneux, D.H., D.R. Hopkins, and N. Zagaria (2004) Disease eradication, elimination and control: the need for accurate and consistent usage. Trends Parasitol, 20(8):347-51.
Nelson K.E and Williams C (2013). Infectious Disease Epidemiology: Theory and Practice. Third edition. Jones and Bartleh Learning
Roberts L, Janovy J (Jr) and Nadler S (2012). Foundations of Parasitology. Ninth edition. McGraw-Hill Publishers, USA.
Schneider M.J (2011). Introduction to Public Health. Third edition. Jones and Bartlett Publishers, Sudbury, Massachusetts, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.