Epidemic disease occurrence refers to the sudden increase in the number of cases of a disease within a specific population, geographic area, or time period beyond what is normally expected. Epidemics can affect human, animal, or plant populations and often result from the interaction of infectious agents, susceptible hosts, and environmental conditions that favor disease transmission. Epidemic disease occurrence is a fundamental aspect of public health, epidemiology, and disease control because epidemics can have significant health, social, and economic consequences on the general population.
The occurrence of an epidemic is influenced by several factors, including the characteristics of the pathogen, host susceptibility, population density, movement of people or animals, environmental changes, and the effectiveness of preventive measures. Infectious diseases such as influenza, cholera, measles, and COVID-19 have demonstrated how rapidly pathogens can spread when favorable conditions exist. In animal populations, epidemic outbreaks can lead to substantial economic losses, particularly in livestock production systems, and may also pose risks to human health through zoonotic transmission.
Epidemic disease occurrence is commonly described using epidemiological measures such as incidence, prevalence, morbidity, and mortality rates. Surveillance systems play a critical role in detecting unusual increases in disease cases, enabling health authorities to identify outbreaks early and implement appropriate interventions. These interventions may include vaccination programs, quarantine measures, improved sanitation, vector control, public awareness campaigns, and antimicrobial treatment where applicable.
The study of epidemic disease occurrence helps researchers and policymakers understand disease patterns, identify risk factors, and develop effective prevention and control strategies. Advances in molecular epidemiology, genomic surveillance, and data analytics have further enhanced the ability to track disease spread and predict potential outbreaks. As globalization, climate change, urbanization, and increased human-animal interactions continue to influence disease dynamics, monitoring and understanding epidemic disease occurrence remain essential for protecting public health and ensuring rapid responses to emerging health threats.
Levels and patterns of disease occurrence
Disease occurrence in a population can be described using several epidemiological terms that indicate the frequency, distribution, and magnitude of a disease within a specific community or geographic area. These levels of disease occurrence is essential for disease surveillance, outbreak detection, public health planning, and the implementation of effective control measures. Epidemiologists use these classifications to determine whether the observed number of disease cases falls within the expected range or represents an unusual increase that requires intervention.
The amount of a particular disease that is consistently present within a population is known as the endemic level or baseline level of disease occurrence. This baseline does not necessarily represent an acceptable or desirable level of disease; rather, it reflects the usual or expected frequency of the disease within a defined population. In some cases, public health authorities may aim to reduce disease occurrence to zero, but until successful interventions are implemented, the disease may continue to persist at its endemic level. Provided that the disease does not exhaust the pool of susceptible individuals and no significant changes occur in environmental or host factors, the disease can remain at this level indefinitely. Consequently, the endemic level serves as a reference point against which changes in disease occurrence are measured.
Certain diseases are extremely rare within a population, making even a single case a cause for immediate concern and epidemiological investigation. Examples include rabies, plague, and poliomyelitis in regions where these diseases have been eliminated or are uncommon. In contrast, diseases such as malaria in some tropical regions or seasonal influenza in many countries occur regularly, and only significant deviations from the normal pattern warrant further investigation.
The term sporadic disease refers to a disease that occurs infrequently and irregularly, with cases appearing at unpredictable intervals and locations. Sporadic cases are generally isolated and do not exhibit a consistent pattern of occurrence. Diseases such as tetanus and certain foodborne infections may occur sporadically when exposure to the causative agent is uncommon.
An endemic disease is one that is constantly present within a particular population or geographic area at a predictable rate. Endemicity does not imply a low disease burden; rather, it indicates a stable and continuous occurrence of disease. For example, malaria remains endemic in many parts of sub-Saharan Africa, where environmental conditions favor the survival and transmission of the mosquito vectors responsible for spreading the disease.
When a disease persists at exceptionally high levels within a population, it is described as hyperendemic. In hyperendemic situations, the disease affects all age groups and continues to occur at a high rate over an extended period. This condition often reflects a sustained interaction between the infectious agent, susceptible hosts, and environmental factors that facilitate transmission. Hyperendemic diseases pose significant public health challenges because they can result in substantial morbidity, mortality, and economic losses.
Occasionally, the number of disease cases rises above the expected endemic level. Such an increase is referred to as an epidemic. An epidemic occurs when the incidence of a disease exceeds what is normally expected in a specific population, area, or time period. Epidemics may result from the introduction of a new pathogen, changes in pathogen virulence, increased host susceptibility, environmental changes, or breakdowns in public health measures. The increase in cases is often sudden and may spread rapidly if effective control measures are not implemented.
The term outbreak is closely related to epidemic and is often used interchangeably. However, outbreak is generally applied to a more localized increase in disease occurrence, such as within a school, hospital, community, or institution. For example, a foodborne illness affecting individuals who attended the same event may be described as an outbreak. Another important epidemiological concept is a cluster, which refers to an aggregation of disease cases grouped in time and place that appears to be greater than expected. In many situations, the expected number of cases may not be known with certainty, but the unusual concentration of cases raises concerns and prompts further investigation. Disease clusters are often examined to determine whether they are linked to a common source of exposure or represent a random occurrence.
The highest level of disease spread is known as a pandemic. A pandemic is an epidemic that extends across multiple countries, continents, or regions of the world and affects a large number of people. Pandemics typically occur when a novel infectious agent emerges and spreads efficiently among populations with little or no pre-existing immunity. One of the most significant recent examples is the COVID-19 pandemic, caused by the SARS-CoV-2 virus, which emerged in late 2019 and rapidly spread worldwide. The pandemic resulted in profound health, economic, and social consequences, highlighting the importance of global disease surveillance, preparedness, and coordinated public health responses.
Factors responsible for epidemic occurrence
An epidemic occurs when the number of disease cases in a population exceeds the expected level within a specific geographic area and time period. Epidemics arise when a disease-causing agent, susceptible hosts, and favorable environmental conditions interact in a manner that promotes rapid disease transmission. The occurrence of an epidemic reflects a disruption in the normal balance between the pathogen, host, and environment, resulting in a sudden increase in disease incidence. Understanding the factors responsible for epidemic occurrence is fundamental to epidemiology because it provides the basis for disease prevention, surveillance, and control strategies.
For an epidemic to occur, three essential components must be present: a causative agent, a susceptible population, and an effective means of transmission. When these components interact under favorable conditions, disease spread can occur rapidly, leading to a significant increase in the number of affected individuals. Epidemics may develop through several mechanisms, each influencing the transmission dynamics of the disease.
One important factor is a recent increase in the amount or virulence of the disease agent. Pathogens can evolve over time through genetic mutation, recombination, or adaptation, resulting in strains that are more infectious, more pathogenic, or more capable of surviving in the environment. An increase in virulence may cause more severe disease manifestations, while an increase in the number of infectious agents may enhance the likelihood of transmission. For example, the emergence of new influenza virus strains has historically been associated with epidemic outbreaks because changes in viral characteristics can increase both infectivity and disease severity.
Another major cause of epidemics is the introduction of an infectious agent into a population where it has not previously existed. When a pathogen enters a new geographical area or a population with little or no prior immunity, large numbers of individuals may become infected within a short period. This situation is particularly common in an increasingly interconnected world where international travel, migration, and global trade facilitate the movement of pathogens across borders. Historical examples include the introduction of smallpox into previously unexposed populations and the global spread of novel infectious diseases such as severe acute respiratory syndrome (SARS), Ebola virus disease, and COVID-19.
Epidemics may also result from an enhanced mode of transmission, which increases the exposure of susceptible individuals to the infectious agent. Changes in environmental conditions, population behavior, sanitation practices, or vector populations can improve the efficiency with which a pathogen spreads. For instance, overcrowded living conditions, inadequate hygiene, contaminated water supplies, and increased human mobility can accelerate disease transmission. Similarly, environmental changes that favor the breeding of disease vectors such as mosquitoes may contribute to outbreaks of malaria, dengue fever, or other vector-borne diseases. When transmission becomes more efficient, even pathogens that previously caused limited disease can generate widespread epidemics.
A change in host susceptibility is another important determinant of epidemic occurrence. The susceptibility of a population can increase when immunity declines, vaccination coverage decreases, nutritional status deteriorates, or underlying health conditions become more prevalent. In populations where immunity is low, infectious agents can spread more readily because a larger proportion of individuals are vulnerable to infection. Demographic factors such as aging populations, population displacement, and the emergence of immunocompromising conditions can also contribute to increased susceptibility. Consequently, diseases that were previously under control may re-emerge and cause epidemics when herd immunity is reduced.
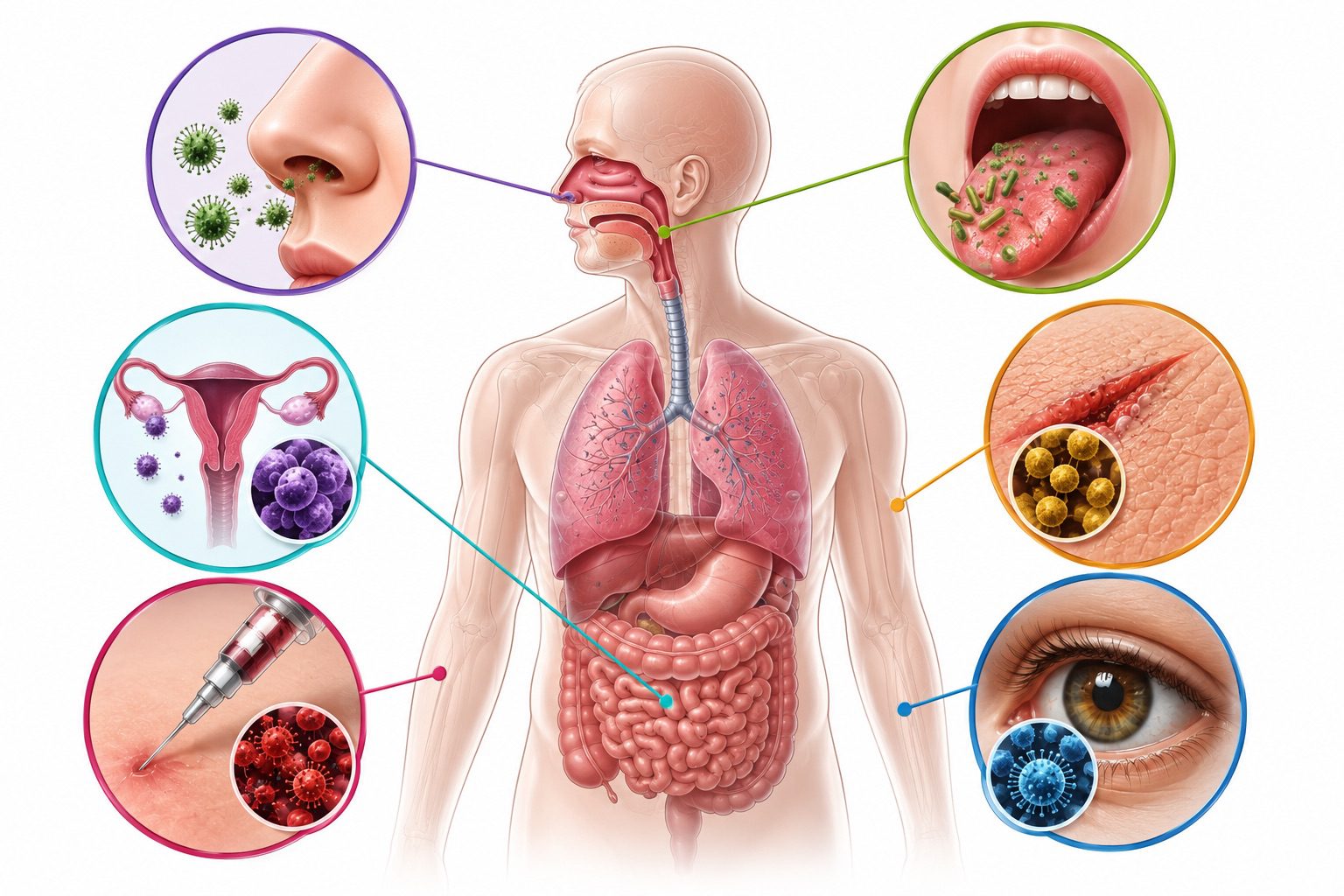
Additionally, epidemics can arise from factors that increase host exposure or introduce pathogens through new portals of entry. Human activities such as urbanization, deforestation, agricultural expansion, and wildlife encroachment can increase contact between humans, animals, and disease reservoirs. These interactions may facilitate the emergence and spread of zoonotic diseases, which are diseases transmitted from animals to humans. Changes in occupational practices, healthcare procedures, food production systems, and environmental management can similarly create new opportunities for pathogen transmission. For example, contaminated medical equipment, unsafe food handling practices, and exposure to polluted water sources can significantly increase the risk of disease outbreaks.
Although epidemics are commonly associated with infectious diseases, the concept of an epidemic is not restricted to infections alone. The term may also be applied to non-communicable diseases and health conditions that occur at unusually high frequencies within populations. In recent decades, chronic diseases such as obesity, diabetes mellitus, cardiovascular diseases, and certain forms of cancer have reached epidemic proportions in many countries. Unlike infectious disease epidemics, these conditions are not transmitted from person to person but are driven by complex interactions among genetic, behavioral, environmental, and socioeconomic factors. Changes in dietary habits, reduced physical activity, urban lifestyles, and increased exposure to risk factors have contributed significantly to the global rise in these diseases.
The global obesity epidemic provides a clear example of how non-infectious diseases can affect large populations and place substantial burdens on healthcare systems. Similarly, the increasing prevalence of diabetes has become a major public health concern worldwide, affecting millions of individuals and contributing to significant morbidity and mortality. These trends demonstrate that epidemic patterns can emerge whenever disease occurrence exceeds expected levels, regardless of whether the underlying condition is infectious or non-infectious.
Epidemics occur when favorable conditions allow a disease agent to spread rapidly among susceptible hosts. Factors such as increased pathogen virulence, introduction of new infectious agents, enhanced transmission mechanisms, increased host susceptibility, and greater exposure opportunities all contribute to epidemic development. Furthermore, the concept of epidemics extends beyond infectious diseases to include chronic health conditions that affect large populations.
Epidemic patterns: modes of disease spread in populations
Epidemics can be classified according to the manner in which disease spreads through a population. Epidemic patterns is a fundamental aspect of epidemiology because it helps investigators identify the source of infection, determine transmission pathways, and implement appropriate control measures. The shape of an epidemic curve, the distribution of cases over time, and the characteristics of affected individuals often provide valuable clues about the underlying pattern of disease spread. Based on these characteristics, epidemics are commonly classified into common-source epidemics, propagated epidemics, mixed epidemics, and other special epidemic patterns.
Common-source outbreaks and their epidemic curves
A common-source outbreak occurs when a group of individuals is exposed to an infectious agent or a toxic substance originating from the same source. The exposure is shared, meaning that all or most cases can be traced back to a single vehicle such as contaminated food, water, air, or an environmental reservoir. Common-source outbreaks are important in epidemiology because they often produce a sudden and identifiable cluster of cases, allowing investigators to rapidly trace the origin of infection and implement control measures to prevent further spread.
In general, common-source outbreaks are characterized by a sharp increase in the number of cases following exposure, especially when the source is clearly identifiable and exposure occurs within a defined setting. Depending on the duration and pattern of exposure, common-source outbreaks are further classified into point-source, continuous-source, and intermittent-source outbreaks. Each type produces a distinct epidemic curve that reflects the timing and intensity of exposure.
A point-source outbreak occurs when a group of people is exposed to the infectious agent or toxin over a very short period of time. In this scenario, exposure is brief and essentially simultaneous for all affected individuals. As a result, all cases develop within a single incubation period of the disease, producing a tightly clustered set of illnesses. The epidemic curve in a point-source outbreak typically shows a rapid and steep increase in cases, followed by a gradual decline as no further exposure occurs and the number of susceptible individuals decreases (Figure 1).
Classic examples of point-source outbreaks include the epidemic of hepatitis A among individuals who consumed contaminated food, such as green onions served at a restaurant in Pennsylvania, and historical radiation-related disease clusters observed following the atomic bomb blast in Hiroshima. In both cases, exposure occurred once or over a very short time frame, and disease onset followed a predictable incubation period pattern. The resulting epidemic curve often resembles a unimodal distribution with a sharp upslope and a more gradual downslope, sometimes described as a “log-normal” shape.
A continuous common-source outbreak occurs when exposure to the infectious agent or toxin persists over an extended period, ranging from several days to weeks or even longer. In this type of outbreak, individuals become exposed at different times, resulting in a wider range of incubation periods. Consequently, the epidemic curve appears flattened and broadened rather than sharply peaked. Instead of a single, well-defined peak, the curve may show a sustained elevation in case numbers over time, reflecting ongoing exposure.
Continuous-source outbreaks are often associated with persistent contamination of a water supply, ongoing exposure to industrial pollutants, or continued distribution of contaminated food products. Because exposure is ongoing, cases continue to appear as long as the source remains active. The control of such outbreaks requires identifying and eliminating the source of contamination to halt further transmission.
An intermittent common-source outbreak occurs when exposure to the infectious agent or toxin is irregular or occurs in repeated episodes over time. In this pattern, individuals are exposed sporadically rather than continuously or all at once. As a result, the epidemic curve often shows multiple peaks or irregular fluctuations corresponding to periods of exposure and non-exposure.
Intermittent outbreaks may occur when contamination of a source is not constant, such as periodic breakdowns in sanitation systems, irregular contamination of food supplies, or episodic release of pathogens into the environment. The irregular nature of exposure makes these outbreaks more difficult to investigate, as identifying the exact timing and source of exposure may require detailed epidemiological analysis and environmental assessment.
The classification of common-source outbreaks into point, continuous, and intermittent types is essential for interpreting epidemic curves and understanding the dynamics of disease transmission. The epidemic curve, which plots the number of cases over time, serves as a key analytical tool in outbreak investigations. It provides insights into the timing of exposure, the incubation period of the disease, and the potential nature of the source.
Common-source outbreaks represent a fundamental pattern of epidemic spread in which individuals are exposed to a shared source of infection or toxin. Whether exposure occurs once, continuously, or intermittently, the resulting epidemic curve provides critical evidence for identifying the source and guiding public health interventions aimed at controlling and preventing further cases.
Propagated epidemics: person-to-person transmission and transmission dynamics
A propagated epidemic is characterized by the progressive spread of an infectious disease from one infected individual to another within a susceptible population. Unlike common-source outbreaks, where individuals are exposed to a single source of infection, propagated outbreaks depend on ongoing chains of transmission. Each infected person may serve as a source of infection for others, leading to successive waves or “generations” of cases over time.
Transmission in propagated epidemics most commonly occurs through direct person-to-person contact. This may involve physical interaction, respiratory droplets, or other forms of close contact that allow the pathogen to move efficiently between hosts. A classic example is syphilis, where transmission occurs primarily through sexual contact. Similarly, many respiratory infections, such as measles or influenza, spread through close interpersonal exposure, particularly in crowded or poorly ventilated environments.
In some cases, propagated transmission occurs indirectly through vehicles or contaminated objects. This is referred to as vehicle-borne transmission, where an inanimate medium carries the infectious agent from one host to another. For instance, hepatitis B virus and human immunodeficiency virus (HIV) can be transmitted through the sharing of contaminated needles or blood products. In these situations, the “vehicle” acts as an intermediary that facilitates infection without requiring immediate person-to-person contact. Propagated epidemics may also involve vector-borne transmission, in which living organisms such as insects transmit the pathogen between hosts. A well-known example is yellow fever, which is transmitted by mosquitoes, particularly Aedes aegypti. In such cases, the vector plays a critical role in maintaining the transmission cycle and expanding the reach of the disease within the population.
A defining feature of propagated epidemics is that cases occur over more than one incubation period of the disease. This means that new waves of cases emerge sequentially as each generation of infections gives rise to the next. The epidemic curve typically shows a series of progressively spaced peaks, each representing a new cycle of transmission (Figure 2). For example, in measles outbreaks, peaks may appear approximately 10-12 days apart, reflecting the incubation period of the virus. This pattern provides important epidemiological evidence of ongoing person-to-person spread rather than a single common exposure.
The progression of a propagated epidemic is influenced by several factors, including the basic reproductive number (R₀), population density, contact patterns, and the level of immunity within the community. When each infected individual transmits the disease to more than one susceptible person, the epidemic expands rapidly. Conversely, when transmission is limited, the outbreak may grow more slowly or decline earlier.
Eventually, a propagated epidemic begins to wane after several generations of transmission. This decline occurs for two primary reasons. First, the number of susceptible individuals in the population decreases as more people become infected and develop immunity, thereby reducing the pool of individuals available for further transmission. Once the proportion of susceptible hosts falls below a critical threshold, sustained transmission becomes difficult. Second, public health interventions such as vaccination campaigns, isolation of cases, contact tracing, improved hygiene, and social distancing measures can significantly reduce transmission rates and interrupt the chain of infection.
Propagated epidemics represent a dynamic and self-sustaining pattern of disease spread driven by sequential transmission between individuals. Their characteristic multi-wave epidemic curves, dependence on incubation periods, and eventual decline due to reduced susceptibility or effective intervention make them a key focus in epidemiological surveillance and infectious disease control. Understanding these patterns enables public health authorities to design timely and targeted responses to limit the impact of outbreaks.
Mixed epidemics: combined common-source and propagated transmission patterns
Mixed epidemics represent outbreak patterns that combine features of both common-source and propagated epidemics. In these situations, an initial wave of cases arises from exposure to a shared source, followed by subsequent waves of disease caused by person-to-person transmission. This dual mechanism of spread makes mixed epidemics particularly important in epidemiology, as they reflect both environmental contamination and ongoing human transmission within a population.
In the early phase of a mixed epidemic, individuals are exposed to a common source of infection. This exposure is typically simultaneous or occurs over a short period, leading to a clustering of cases within a defined time frame. The common source may include contaminated food or water, environmental exposure, or a shared event where infected material is present. As a result, a sharp increase in cases is often observed shortly after exposure, resembling a point-source epidemic curve.
However, unlike purely common-source outbreaks, mixed epidemics do not end after the initial exposure is removed. Instead, they transition into a second phase characterized by propagated spread, in which infected individuals transmit the pathogen directly to others. This leads to secondary, tertiary, and sometimes further generations of cases. The epidemic curve in this stage typically shows multiple peaks or a prolonged tail, reflecting successive waves of transmission within the population.
The development of a mixed epidemic depends on several factors, including the infectiousness of the agent, the incubation period, population density, and the effectiveness of control measures. Pathogens that are easily transmitted from person to person, especially those with short incubation periods and high environmental stability, are more likely to produce mixed epidemic patterns. Additionally, delays in outbreak detection or intervention can allow secondary transmission to become well established.
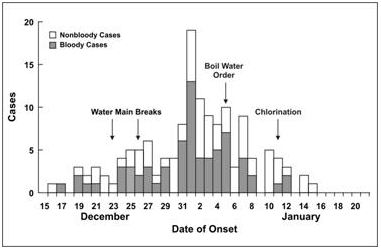
A classic example of a mixed epidemic is a shigellosis outbreak that occurred among approximately 3,000 women attending a national music festival (Figure 3). During the event, many attendees were exposed to a contaminated source, leading to a large number of primary cases. After returning to their home communities, these individuals developed symptoms of shigellosis caused by Shigella infection. This initial common-source outbreak was subsequently followed by secondary transmission.
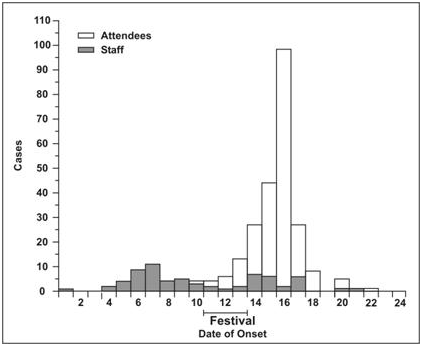
Over the following weeks, several state health departments identified additional cases that were not directly linked to the festival itself but were instead associated with household and community contact with infected individuals. These later cases represented person-to-person spread, demonstrating the propagated component of the outbreak. The combination of a large initial exposure event and ongoing transmission resulted in a sustained epidemic across multiple geographic regions.
Mixed epidemics present unique challenges for public health response because control measures must address both the original source of infection and the mechanisms of secondary transmission. Eliminating the source alone is often insufficient if person-to-person spread continues within the community. Therefore, interventions such as isolation of cases, hygiene promotion, contact tracing, and community education are essential to interrupt transmission chains. Mixed epidemics illustrate the complex nature of disease spread in real-world settings. By combining elements of common-source exposure and propagated transmission, they highlight the importance of comprehensive surveillance and multifaceted control strategies in managing infectious disease outbreaks.
Zoonotic and vector-borne epidemic patterns: ecological transmission cycles
Not all epidemics conform to the classical frameworks of common-source or propagated (person-to-person) transmission. A distinct category of epidemic pattern arises from zoonotic and vector-borne diseases, in which transmission depends on ecological interactions among wildlife reservoirs, arthropod vectors, and human populations. In these outbreaks, humans are typically incidental or “dead-end” hosts, and sustained human-to-human transmission is absent or minimal. Instead, epidemic emergence is driven by ecological amplification processes involving reservoir hosts, vector abundance, and environmental conditions that facilitate human exposure.
These epidemics occur when there is sufficient prevalence of infection in reservoir host species, a sufficient density of competent vectors, and increased human-vector or human-environment interaction. The convergence of these factors allows pathogens maintained in animal populations to spill over into humans at levels high enough to produce recognizable outbreaks or epidemics. Unlike common-source outbreaks, where a single contaminated source may be identified, or propagated outbreaks, where transmission occurs directly between humans, zoonotic and vector-borne epidemics are embedded in complex ecological systems.
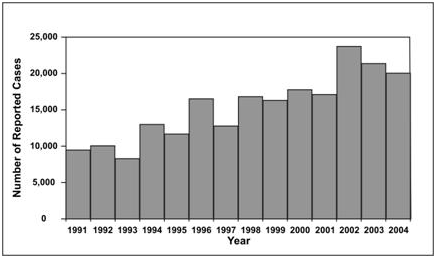
A classic example is the emergence of Lyme disease in the northeastern United States during the late 1980s (Figure 4). Lyme disease is caused by the bacterium Borrelia burgdorferi and is transmitted to humans through the bite of infected deer ticks (Ixodes species). The epidemic was not the result of direct human-to-human transmission, but rather an ecological imbalance involving deer populations, small mammal reservoirs (particularly mice), and expanding tick populations. As suburban development increasingly encroached on forested areas, human exposure to tick habitats increased significantly. Deer served as key hosts for adult ticks, supporting tick reproduction and population expansion, while infected small mammals maintained the bacterial reservoir. The result was a sustained increase in human cases, forming a recognizable epidemic pattern driven by ecological conditions rather than direct transmission chains.
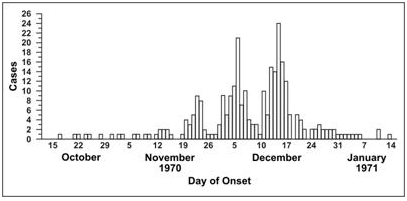
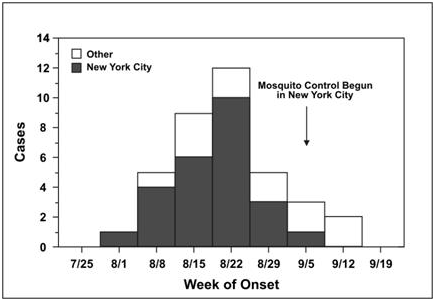
Similarly, the outbreak of West Nile encephalitis in the Queens section of New York City in 1999 illustrates another vector-borne epidemic pattern (Figure 5). West Nile virus is primarily maintained in a transmission cycle between birds and mosquitoes. Humans and other mammals become infected incidentally when bitten by infected mosquitoes, particularly species of Culex. The 1999 outbreak was initially detected through unusual clusters of severe neurological illness in humans, along with concurrent die-offs in bird populations, especially crows. Environmental conditions, including warm temperatures and urban mosquito breeding habitats, contributed to increased vector abundance and intensified transmission. Although humans were significantly affected, they did not contribute substantially to onward transmission, highlighting the role of ecological amplification rather than direct human spread.
These zoonotic and vector-borne epidemic patterns underscore the importance of ecosystem dynamics in disease emergence. Factors such as climate variability, land-use change, urbanization, biodiversity loss, and wildlife population shifts can all influence the balance between pathogens, vectors, and hosts. Small changes in any component of this system can significantly alter transmission intensity, potentially triggering outbreaks.
From a public health perspective, controlling these epidemics requires strategies that extend beyond treating human cases. Effective interventions often target multiple levels of the transmission cycle, including vector control (e.g., insecticide use and habitat reduction), reservoir host management, environmental modification, and reduction of human exposure to high-risk areas. Surveillance systems that integrate veterinary, entomological, and environmental data often described under the One Health approach are essential for early detection and prevention.
Zoonotic and vector-borne epidemics represent environmentally driven disease patterns in which human infection results from complex interactions among wildlife reservoirs, arthropod vectors, and ecological conditions. The Lyme disease and West Nile virus outbreaks demonstrate how changes in ecosystems can translate into significant human disease burdens.
Source
Balows A, Hausler W, Herrmann K.L, Isenberg H.D and Shadomy H.J (1991). Manual of clinical microbiology. 5th ed. American Society of Microbiology Press, USA.
Bonita R., Beaglehole R., Kjellström T (2006). Basic epidemiology. 2nd edition. World Health Organization. Pp. 1-226.
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA.
Castillo-Salgado C (2010). Trends and directions of global public health surveillance. Epidemiol Rev, 32:93–109.
Center for Disease Control and Prevention
Porta M (2008). A dictionary of epidemiology. 5th edition. New York: Oxford University Press.
Rothman K.J and Greenland S (1998). Modern epidemiology, 2nd edition. Philadelphia: Lippincott-Raven.
Rothman K.J, Greenland S and Lash T.L (2011). Modern Epidemiology. Third edition. Lippincott Williams and Wilkins, Philadelphia, PA, USA.
www.cdc.gov/csels/dsepd/ss1978/lesson1/section11.html
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.