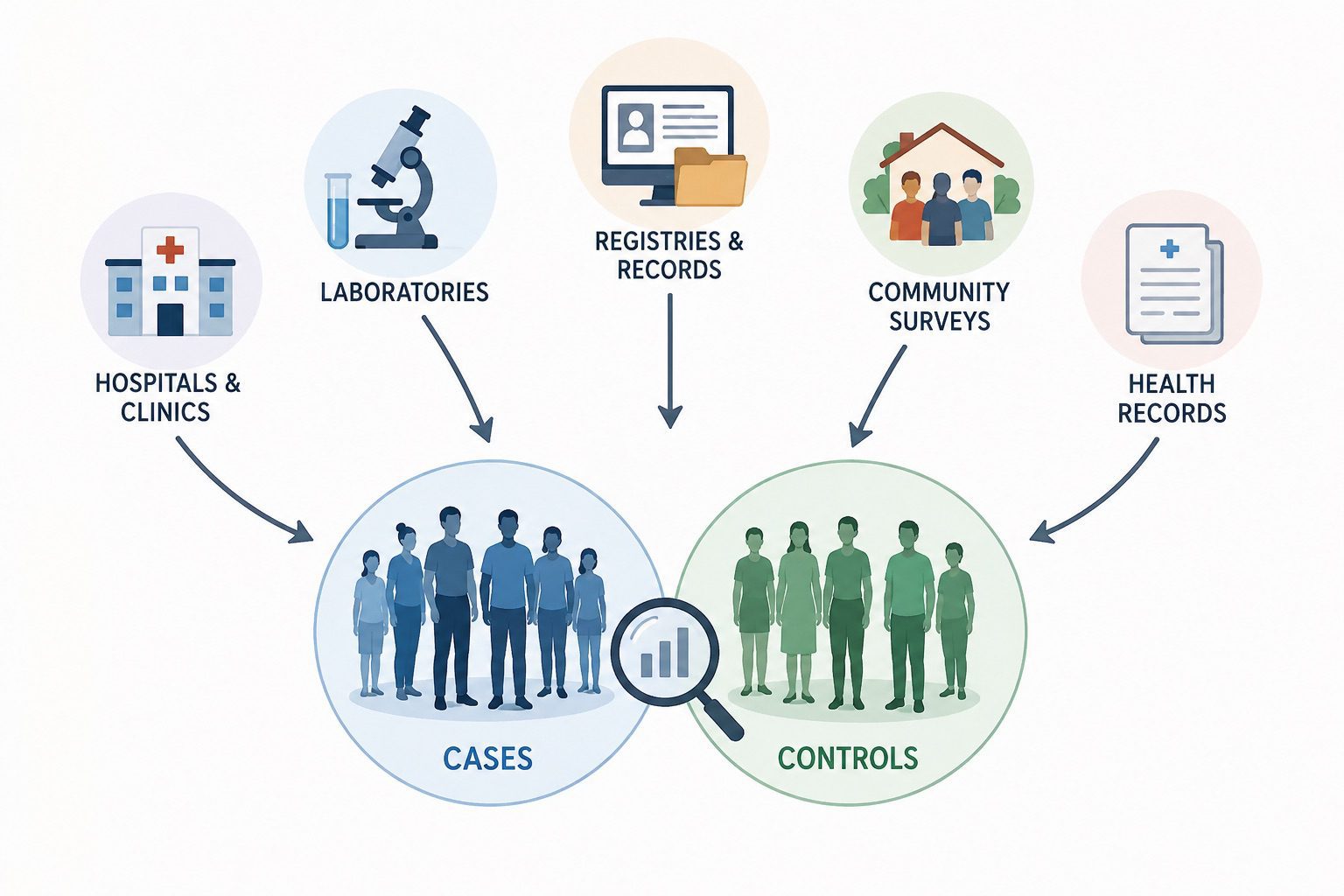
In epidemiological research, particularly in case-control studies, the selection of cases and controls is one of the most critical methodological steps because it directly influences the validity and reliability of study findings. Cases are individuals who have the disease, condition, or outcome of interest, whereas controls are individuals who do not have the outcome but are otherwise representative of the population from which the cases arose. The fundamental principle is that both cases and controls should originate from the same source population so that any observed differences in exposure can be attributed to factors associated with the disease rather than to selection bias.
Cases can be obtained from a variety of sources depending on the study objectives, disease characteristics, and available resources. One common source is hospitals and healthcare facilities, where patients diagnosed with a particular disease are identified through medical records, diagnostic registers, or specialist clinics. Hospital-based cases are often easy to access and provide confirmed diagnoses; however, they may not represent all individuals with the disease in the wider community, particularly when access to healthcare is uneven. Another important source is disease registries, which systematically collect information on specific diseases such as cancer, tuberculosis, or congenital disorders. Registries are valuable because they often provide comprehensive coverage of diagnosed cases within a defined population and time period.
Community-based case identification is another approach, especially for diseases that may not always result in hospitalization. Cases may be detected through household surveys, community screening programs, or active surveillance systems. This method is particularly useful in public health studies where researchers seek to capture both diagnosed and undiagnosed cases. Laboratory databases can also serve as sources of cases, especially for infectious diseases where diagnosis is confirmed through microbiological, molecular, or serological testing. In some studies, cases may be identified through health insurance records, occupational health databases, or electronic health records, which provide access to large populations and extensive health information.
Controls must be selected carefully because they provide the baseline against which exposures among cases are compared. Ideally, controls should be representative of the population that produced the cases and should have had the same opportunity to be exposed to the risk factors under investigation. One common source of controls is the general population. Population-based controls may be selected from census records, voter registration lists, household surveys, or other population databases. These controls are often preferred because they are more likely to represent the exposure distribution in the source population.
Hospital controls are another frequently used source. These are patients admitted to the same hospitals as the cases but for conditions unrelated to the exposure being studied. Hospital controls can be convenient and cost-effective because they are readily available and often willing to participate. However, researchers must ensure that the illnesses affecting these controls are not associated with the exposure of interest, as this could introduce bias into the study.
Neighborhood or community controls may also be selected, particularly when cases are identified from a specific geographic area. These controls are often matched to cases on factors such as age, sex, or place of residence to reduce confounding. Friends, relatives, or coworkers of cases have sometimes been used as controls because they are easy to recruit and may share similar social characteristics. Nevertheless, such controls may have exposure patterns that are too similar to those of cases, potentially reducing the ability of the study to detect meaningful associations.
Specialized studies may obtain controls from schools, workplaces, healthcare databases, or occupational registries, depending on the target population. Regardless of the source, the key requirement is that controls should accurately reflect the exposure experience of the population at risk from which the cases emerged. Careful selection of both cases and controls minimizes selection bias, improves comparability between groups, and strengthens the credibility of conclusions regarding the relationship between exposure and disease. Consequently, identifying appropriate sources of cases and controls is a cornerstone of sound epidemiological study design and essential for generating valid and interpretable results.
Importance of sources of cases and controls in an epidemiological study
Selecting appropriate sources ensures efficient use of resources by facilitating data collection, improving participant recruitment, and enhancing the quality of information obtained. Reliable case and control selection contributes to accurate estimation of disease risk factors, supports evidence-based decision-making, and ultimately strengthens the scientific value of epidemiological investigations. Therefore, identifying suitable sources of cases and controls is a critical step in conducting valid and meaningful epidemiological studies.
The selection of appropriate sources of cases and controls is one of the most important aspects of epidemiological research, particularly in case-control studies. Cases and controls form the foundation upon which comparisons are made to determine whether a particular exposure is associated with a disease or health outcome. Consequently, the validity, reliability, and credibility of study findings depend largely on how these groups are selected.
One major importance of carefully selecting sources of cases and controls is the reduction of selection bias. Cases should accurately represent individuals with the disease in the target population, while controls should represent the population from which the cases arose. If either group is selected from inappropriate sources, the observed relationship between exposure and disease may be distorted, leading to incorrect conclusions.
Appropriate sources of cases and controls also improve the comparability between the two groups. Controls should have characteristics similar to those of cases, except for the presence of the disease under investigation. When cases and controls come from the same source population, differences in exposure are more likely to reflect true associations rather than differences arising from the selection process.
Another important benefit is the enhancement of the internal validity of the study. Internal validity refers to the extent to which the study accurately measures the relationship between exposure and disease. Properly selected cases and controls minimize systematic errors and strengthen confidence in the study findings.
The choice of suitable sources also improves the generalizability or external validity of research results. Cases and controls drawn from representative populations make it easier to apply study findings to broader populations and settings. This is particularly important in public health research, where findings are often used to guide disease prevention and control strategies.
Sources of cases in an epidemiological study
The identification and selection of cases are fundamental steps in epidemiological research, particularly in case-control studies. As aforesaid, a case refers to an individual who has the disease, health condition, or outcome of interest being investigated. The validity of a study largely depends on how accurately and systematically cases are identified. Therefore, researchers must use reliable sources that ensure cases truly represent the population affected by the disease under investigation. Cases can be obtained from several sources depending on the study design, disease characteristics, available resources, and the objectives of the research. The following are some of the most important sources of cases in an epidemiological study:
1. Cases obtained from hospital registries, clinics, and disease screening records
One of the most common sources of cases is healthcare facilities such as hospitals, clinics, and disease screening centers. Researchers can identify cases through hospital registries, patient medical records, outpatient clinics, specialized treatment centers, and disease screening programs. These sources are particularly useful because diagnoses are often confirmed by qualified healthcare professionals using standardized diagnostic procedures.
Hospital records provide detailed information on patients’ medical histories, clinical findings, laboratory results, and treatment outcomes. Similarly, disease screening programs can identify individuals with specific conditions at an early stage, even before symptoms become severe. This source is especially valuable for studies investigating chronic diseases such as cancer, diabetes, hypertension, and infectious diseases. However, researchers should be aware that hospital-based cases may not fully represent all cases in the general population, particularly in areas where access to healthcare services is limited.
2. All cases diagnosed in a particular hospital department at a given time
Cases may also be selected from a specific hospital department within a defined period. For example, a researcher studying breast cancer may include all patients diagnosed in the oncology department of a hospital between January and December of a particular year. This approach allows researchers to obtain a clearly defined group of cases and facilitates efficient data collection.
Using cases from a particular department is often practical and cost-effective because the cases are concentrated in one location and their medical records are readily available. In addition, diagnoses are usually consistent because they are made by specialists within the same department. Nevertheless, such cases may not represent patients treated elsewhere or individuals who never seek medical care, which could limit the generalizability of study findings.
3. All cases diagnosed in the community or population
Another important source of cases is the community or the general population. In population-based studies, researchers attempt to identify all individuals with the disease within a defined geographic area or population group. Cases may be identified through community surveys, household visits, active surveillance systems, health campaigns, or disease notification systems.
Community-based case identification is advantageous because it captures both hospitalized and non-hospitalized individuals, thereby providing a more accurate representation of disease occurrence in the population. This method is particularly useful for conditions that do not always require hospital admission or for diseases that may be underreported in healthcare facilities. Although community-based studies often provide highly representative data, they can be time-consuming, expensive, and logistically challenging to conduct.
4. All cases diagnosed in all hospitals (public and private)
Researchers may also obtain cases from all hospitals within a particular area, including both public and private healthcare institutions. This approach broadens the coverage of case identification and reduces the likelihood of missing cases that seek care in different health facilities. It is especially useful for studying relatively rare diseases where a large number of cases is required.
By including cases from multiple hospitals, researchers can increase the representativeness of the study population and improve the external validity of the findings. Furthermore, this method minimizes selection bias that may occur when cases are drawn from a single healthcare institution. However, researchers must ensure that consistent diagnostic criteria are applied across all participating hospitals to maintain data quality and comparability.
5. All cases diagnosed in a sample or fraction of the population
In some situations, it may not be feasible to identify every case within an entire population due to financial, logistical, or time constraints. Researchers may therefore select cases from a representative sample or fraction of the population. This approach involves identifying cases within a carefully chosen subset of the population that reflects the characteristics of the larger community.
Sampling methods such as random sampling, cluster sampling, or stratified sampling may be used to ensure that the selected cases are representative. When conducted properly, this approach can provide reliable and valid estimates while reducing study costs and workload. However, the accuracy of the findings depends on the quality of the sampling procedure and the extent to which the sample reflects the target population.
Cases in epidemiological studies can be sourced from hospitals, clinics, disease registries, specific hospital departments, community populations, multiple healthcare institutions, or representative samples of the population. The choice of source depends on the study objectives, available resources, and the need to obtain cases that accurately represent the population affected by the disease. Careful case selection is essential for minimizing bias and ensuring the validity of epidemiological research findings.
Sources of controls in an epidemiological study
In epidemiological research, particularly in case-control studies, the selection of appropriate controls is as important as the selection of cases. Controls are individuals who do not have the disease or outcome under investigation but who originate from the same source population as the cases. They serve as the comparison group against which the exposure histories of cases are evaluated. The primary purpose of selecting controls is to estimate the frequency of exposure among individuals who could have become cases but did not develop the disease. Therefore, controls should be representative of the population from which the cases arose and should have had a similar opportunity for exposure to the risk factors being studied.
The validity of a case-control study depends heavily on the proper selection of controls. If controls are not representative of the source population, selection bias may occur, leading to inaccurate conclusions about the association between exposure and disease. Consequently, epidemiologists carefully choose controls from sources that provide the greatest comparability with cases while minimizing bias and confounding. The following are some of the most important sources of controls in an epidemiological study:
1. Samples of patients who do not have the disease under study in all hospitals
One common source of controls is patients attending hospitals who do not have the disease being investigated. These individuals may be selected from various hospitals within the study area, including both public and private healthcare facilities. Such controls are often referred to as hospital controls.
Hospital controls are advantageous because they are usually readily available, easy to recruit, and often willing to participate in research. Their medical records may also provide valuable information on demographic characteristics and exposure histories. Furthermore, because they are drawn from healthcare facilities, they may have similar healthcare-seeking behaviors as the cases.
However, researchers must exercise caution when selecting hospital controls. The illnesses affecting these individuals should not be related to the exposure being studied; otherwise, the exposure distribution among controls may not accurately represent that of the source population. For example, if smoking is the exposure of interest in a lung cancer study, selecting controls with smoking-related diseases could lead to biased results.
2. Samples from members of the general community or population at risk
Another important source of controls is the general population from which the cases originate. These population-based controls are selected from individuals who are at risk of developing the disease but have not done so. They may be identified through household surveys, census records, voter registration lists, community databases, or other population registers.
Population controls are often considered ideal because they are more likely to reflect the true distribution of exposures in the source population. They provide a broader representation of the community and are particularly useful when cases are also population-based. This approach enhances the external validity and generalizability of study findings.
Despite these advantages, recruiting population controls can be expensive, time-consuming, and logistically challenging. Researchers may need extensive resources to locate, contact, and interview participants, particularly in large or geographically dispersed populations.
3. Relations, spouses, children, or companions of the cases
In some epidemiological studies, controls are selected from among the relatives, spouses, children, friends, or companions of cases. This method is often used because such individuals are readily accessible and may be more willing to participate in the study. A major advantage of using relatives or companions as controls is that they often share similar socioeconomic backgrounds, environmental conditions, cultural practices, and healthcare access with the cases. These similarities can help reduce the influence of certain confounding factors.
However, this source of controls may introduce bias because family members and close associates frequently share similar exposure patterns. If the exposure of interest is common within families or households, the differences between cases and controls may be minimized, making it more difficult to detect a true association between exposure and disease. Consequently, researchers must carefully evaluate whether this type of control group is appropriate for the specific study.
4. Samples of patients in the same hospital where cases were obtained
Controls may also be selected from the same hospital in which the cases were identified, provided that they do not have the disease under investigation. This approach is widely used in hospital-based case-control studies because it ensures that cases and controls come from a similar healthcare environment.
Selecting controls from the same hospital offers several practical advantages. Data collection is often easier, recruitment costs are lower, and information can be obtained using similar procedures for both groups. Additionally, cases and controls may be more comparable with respect to healthcare utilization and referral patterns. Nevertheless, the diseases affecting the controls must be unrelated to the exposure under investigation. Failure to consider this issue can result in selection bias and distorted estimates of disease risk.
5. Non-cases in a sample of the community or population
Another valuable source of controls is non-cases identified within a representative sample of the community or population. Researchers may conduct surveys or screening programs to identify individuals who do not have the disease but who belong to the same population from which cases arose. These controls are particularly useful in population-based epidemiological studies because they provide an accurate reflection of the exposure experience within the community. Sampling methods such as random sampling, stratified sampling, or cluster sampling are often employed to ensure representativeness.
Although community-based controls generally improve the validity of study findings, identifying and recruiting them can require substantial financial resources, personnel, and time. Despite these challenges, they are often preferred when the goal is to obtain controls that closely mirror the population at risk.
Controls in epidemiological studies can be obtained from hospital patients without the disease, members of the general population at risk, relatives or companions of cases, patients from the same hospital where cases are identified, or non-cases selected from community samples. Regardless of the source, the essential requirement is that controls should represent the population that gave rise to the cases and should have had a similar opportunity for exposure to the risk factors under investigation. Careful control selection reduces bias, improves comparability between study groups, and enhances the validity of conclusions regarding the relationship between exposure and disease.
References
Aschengrau A and Seage G.R (2013). Essentials of Epidemiology in Public Health. Third edition. Jones and Bartleh Learning,
Aschengrau, A., & G. R. Seage III. (2009). Essentials of Epidemiology in Public Health. Boston: Jones and Bartlett Publishers.
Bonita R., Beaglehole R., Kjellström T (2006). Basic epidemiology. 2nd edition. World Health Organization. Pp. 1-226.
Porta M (2008). A dictionary of epidemiology. 5th edition. New York: Oxford University Press.
Rothman K.J and Greenland S (1998). Modern epidemiology, 2nd edition. Philadelphia: Lippincott-Raven.
Rothman K.J, Greenland S and Lash T.L (2011). Modern Epidemiology. Third edition. Lippincott Williams and Wilkins, Philadelphia, PA, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.