
Anthroponotic diseases (anthroponoses) and sapronoses represent two distinct ecological and epidemiological modes of infectious disease transmission, defined primarily by the nature of their reservoirs and the pathways through which pathogens are maintained and propagated in the environment. They expand the classical human-animal framework of infectious disease ecology by emphasizing the roles of human-to-human maintenance systems and abiotic environmental reservoirs, respectively. A good knowledge of anthroponoses and sapronoses is central to modern epidemiology, particularly in the context of emerging infections, antimicrobial resistance dissemination, and environmental health interactions.
In anthroponotic systems, humans function as the primary and often exclusive reservoir for infectious agents. This implies that pathogen persistence does not depend on non-human hosts or environmental reservoirs but is sustained through chains of transmission among human populations. Such systems are particularly important in densely populated settings where social contact rates are high, enabling efficient propagation of infectious agents. From a population biology perspective, anthroponotic pathogens are strongly shaped by human demography, mobility, hygiene infrastructure, and behavioral patterns. Their evolutionary trajectories are often characterized by adaptation to human-specific physiological conditions and immune pressures, leading to specialized host-pathogen interactions. The epidemiological consequence is that control strategies targeting human behavior, vaccination, sanitation, and case isolation can, in principle, interrupt transmission entirely because the reservoir is self-contained within the human population.
Sapronotic systems are defined by the maintenance of pathogens in abiotic environmental substrates such as soil, water, decaying organic matter, or built environments, independent of vertebrate hosts. In these systems, the environment itself acts as the ecological reservoir where pathogens can survive, persist, and in some cases replicate. Human infection occurs through incidental exposure to contaminated environmental sources rather than through sustained person-to-person transmission cycles. This ecological arrangement introduces a fundamentally different dynamic, as pathogen persistence is decoupled from host population structure and instead governed by environmental conditions such as temperature, moisture, nutrient availability, and physicochemical stability. As a result, sapronotic agents often exhibit broad environmental tolerance and may possess adaptive traits enabling long-term survival outside a host, including biofilm formation or resistance to desiccation and UV radiation.
The distinction between these two transmission modes has profound implications for disease control and public health strategy. In anthroponotic systems, interventions can be highly targeted at human populations, since breaking transmission chains directly reduces or eliminates the pathogen reservoir. In sapronotic systems, however, interventions must extend beyond human hosts to include environmental management, such as water treatment, soil decontamination, or control of industrial and domestic ecological niches that support pathogen persistence. This introduces additional complexity, as complete environmental eradication is often impractical, and exposure risk may persist even in the absence of infected individuals.
Both anthroponotic and sapronotic frameworks are increasingly relevant in the context of global environmental change and antimicrobial resistance. Environmental reservoirs can serve as long-term storage sites for resistance determinants, while dense human populations and global travel networks facilitate rapid anthroponotic spread. The interplay between these systems highlights the importance of integrated One Health approaches that consider human, environmental, and microbial ecology as interconnected components of disease dynamics.
Anthroponoses: human-restricted infectious diseases maintained through human-to-human transmission
An anthroponosis is an infectious disease caused by a pathogen whose primary reservoir is humans and whose transmission occurs predominantly between humans, without requiring an animal or environmental reservoir for its long-term maintenance. In anthroponotic diseases, infected individuals serve as the principal source of infection for other susceptible people, enabling the pathogen to persist within human populations through continuous transmission cycles. These diseases are maintained through direct person-to-person contact or indirect routes such as respiratory droplets, bodily fluids, contaminated food or water, or vectors that acquire the pathogen from infected humans.
Unlike zoonoses and sapronoses, anthroponoses depend largely on human hosts for survival, reproduction, and dissemination. The epidemiology of anthroponotic diseases is therefore strongly influenced by human population density, mobility, social interactions, sanitation, and healthcare practices. Many important public health threats, including several viral, bacterial, and parasitic infections, are classified as anthroponoses because humans constitute their essential reservoir. Effective control strategies often focus on interrupting transmission between people through vaccination, surveillance, treatment, hygiene measures, and public health interventions. Understanding anthroponoses is fundamental to infectious disease management because their persistence is directly linked to human behavior and population dynamics.
Characteristics of anthroponoses
The following are key characteristics of anthroponotic disease:
- Humans as the primary reservoir
- The pathogen is naturally maintained within human populations and relies on humans as its principal host.
- Predominant human-to-human transmission
- Infection spreads mainly from one person to another through direct or indirect transmission pathways.
- Dependence on human hosts for persistence
- The pathogen requires continuous circulation among humans to sustain its presence over time.
- Absence of an essential animal reservoir
- Unlike zoonotic diseases, anthroponotic pathogens do not depend on animal populations for their long-term maintenance.
- Potential for sustained epidemics
- Continuous human-to-human transmission can facilitate outbreaks, epidemics, or pandemics in susceptible populations.
- Transmission through multiple routes
- Spread may occur via respiratory droplets, aerosols, physical contact, sexual contact, bodily fluids, contaminated food or water, or human-associated vectors.
- Influence of human demographics and behavior
- Population density, migration, urbanization, travel, hygiene practices, and social interactions significantly affect disease transmission.
- Control through public health measures
- Vaccination, isolation, treatment, contact tracing, sanitation improvements, and health education are often effective strategies for disease prevention and control.
- Pathogen adaptation to human hosts
- Many anthroponotic pathogens exhibit a high degree of adaptation to human physiology and immune systems.
- Global public health importance
- Because humans are both the reservoir and the susceptible population, anthroponoses can spread rapidly across communities and international borders.
Examples of anthroponotic diseases
Examples of anthroponoses include: Measles, which is maintained exclusively through human-to-human transmission, as well as Rubella, Mumps, Pertussis, Diphtheria, and Typhoid fever, all of which rely primarily on human reservoirs for their persistence and spread. Other notable anthroponotic diseases include Poliomyelitis, Gonorrhea, Syphilis,and AIDS, which are sustained predominantly through transmission among human populations. Some parasitic diseases, such as Malaria caused by Plasmodium falciparum, Amoebiasis, and Trichomoniasis, are also considered anthroponotic because humans serve as the principal reservoir, while vectors or environmental stages may facilitate transmission without acting as long-term reservoir hosts.
Sapronosis: environmentally maintained infectious diseases originating from non-living reservoirs
A sapronosis is an infectious disease caused by a pathogen that naturally lives, reproduces, and persists in an abiotic (non-living) environment, such as soil, water, sediment, or decaying organic matter, rather than requiring a living host for its survival and multiplication. Unlike many infectious diseases that depend on humans, animals, or plants as primary reservoirs, sapronotic pathogens complete a substantial part of their life cycle in environmental substrates. These microorganisms are typically free-living and possess the ability to grow and multiply independently in nature. Human or animal infection occurs when individuals come into contact with contaminated environmental sources through inhalation, ingestion, skin contact, or traumatic inoculation.
The environmental reservoir therefore serves not merely as a temporary habitat but as the principal source of pathogen maintenance and propagation. Sapronoses are commonly associated with fungi, bacteria, and some protozoa that thrive under favorable environmental conditions. Their occurrence is often influenced by ecological factors such as temperature, moisture, nutrient availability, and organic matter decomposition. Understanding sapronoses is particularly important within the One Health framework because environmental changes, land use practices, and climate variability can significantly affect pathogen persistence and transmission dynamics.
Examples of sapronotic diseases
Key examples of sapronotic diseases include: Legionnaires’ disease, caused by Legionella spp. that proliferate in natural and man-made aquatic environments such as freshwater systems, cooling towers, and plumbing networks; Histoplasmosis, caused by Histoplasma capsulatum, and acquired through inhalation of fungal spores originating from soil enriched with bird or bat droppings; Coccidioidomycosis, caused by Coccidioides spp., and resulting from inhalation of airborne Coccidioides spores dispersed from arid and semi-arid soils; Blastomycosis, caused by Blastomyces spp. inhabiting moist soils and decaying organic matter; Cryptococcosis, associated with environmental exposure to Cryptococcus spp. present in soil, decaying wood, and bird-associated habitats; Melioidosis, caused by Burkholderia pseudomallei, a soil- and water-dwelling bacterium commonly found in tropical and subtropical regions; Aspergillosis, which arises from inhalation of Aspergillus spores originating from soil, compost, and decaying vegetation, and Primary amoebic meningoencephalitis, a rare but severe infection caused by the free-living amoeba Naegleria fowleri inhabiting warm freshwater environments.
Characteristics of sapronoses
The following are the key characteristics of sapronotic diseases:
- Abiotic environmental reservoir
- The pathogen is maintained primarily in non-living environmental habitats such as soil, water, sediments, compost, or decaying vegetation.
- Independent environmental multiplication
- Unlike many zoonotic pathogens, sapronotic agents can actively grow and reproduce outside a living host.
- Host not essential for survival
- Human or animal hosts are incidental and generally not required for the long-term persistence of the pathogen in nature.
- Environmental exposure as the main route of infection
- Transmission typically occurs through contact with contaminated environmental sources rather than direct host-to-host spread.
- Strong influence of environmental conditions
- Factors such as temperature, humidity, pH, nutrient availability, and organic matter content strongly affect pathogen survival and proliferation.
- Limited or absent person-to-person transmission
- Most sapronoses are acquired directly from the environment, with secondary transmission between infected hosts being uncommon or nonexistent.
- Association with free-living microorganisms
- Many sapronotic pathogens are naturally occurring environmental microbes that can opportunistically infect humans or animals under suitable conditions.
- Ecological and climatic sensitivity
- Changes in climate, land use, agricultural practices, and ecosystem disturbances can alter the distribution and abundance of sapronotic pathogens.
- Often opportunistic in nature
- Infection frequently occurs in individuals with increased susceptibility, although some sapronotic pathogens can also infect healthy hosts.
- Importance in environmental and public health
- Prevention and control strategies often focus on environmental management and exposure reduction rather than interruption of host-to-host transmission.
Human and animal reservoirs in the continuum of infectious disease transmission
Anthroponotic diseases (anthroponoses) and zoonotic diseases (zoonoses) represent two tightly connected but ecologically distinct components of infectious disease transmission systems, unified by the movement of pathogens across host species boundaries. Their relationship is best understood through the concept of reservoirs and transmission directionality, where the primary distinction lies in whether humans or animals function as the dominant maintenance host. In anthroponoses, humans serve as the principal reservoir, sustaining the pathogen through continuous human-to-human transmission cycles. In zoonoses, animals are the principal reservoir, with humans acting as incidental or spillover hosts. Despite this distinction, both systems are dynamically linked through bidirectional interfaces between human populations and animal ecosystems.
The linkage between anthroponoses and zoonoses becomes evident when considering that many pathogens do not remain confined to a single host category over evolutionary time. Instead, they may transition between animal and human reservoirs depending on ecological pressures, host density, and opportunities for cross-species transmission. Zoonotic pathogens, in particular, are a major source of newly emerging anthroponotic infections. When a pathogen originally maintained in animals acquires the ability to sustain human-to-human transmission, it effectively shifts from a zoonotic cycle into an anthroponotic one. This transition represents a critical evolutionary step in pathogen adaptation, as it requires overcoming barriers related to host specificity, immune evasion, and efficient transmission among humans.
On the other hand, anthroponotic systems can also interact with animal populations, creating spillback events where human-adapted pathogens are transmitted to animals. While these spillovers may not always establish sustained transmission in animal hosts, they demonstrate the porous nature of host boundaries. In certain cases, however, such reverse transmission can lead to the establishment of secondary reservoirs in animals, potentially reintroducing pathogens into human populations at later stages. This bidirectional exchange highlights the ecological continuity between anthroponotic and zoonotic systems rather than their strict separation (Figure 1).
At the population level, the stability of anthroponotic transmission depends on sustained chains of human-to-human contact, whereas zoonotic stability depends on the persistence of infection within animal reservoirs. However, these systems are not isolated; they often intersect through shared environments, vectors, and interfaces such as domestic animals, wildlife contact zones, and agricultural systems. These interfaces function as ecological bridges, enabling pathogens to move between anthroponotic and zoonotic cycles. As a result, disease emergence is frequently driven by perturbations at the human-animal interface, including habitat encroachment, domestication practices, and global trade in animals and animal products.
A central feature linking both categories is the concept of the “spillover event,” were pathogens cross species barriers. In zoonoses, spillover represents the initial transmission from animals to humans. In anthroponoses, sustained human-to-human transmission following spillover represents the establishment phase of a new epidemiological system. This continuum underscores that anthroponotic diseases can often be viewed as zoonotic-origin infections that have achieved full adaptation to humans, while zoonotic diseases represent those that remain dependent on animal reservoirs for long-term maintenance.
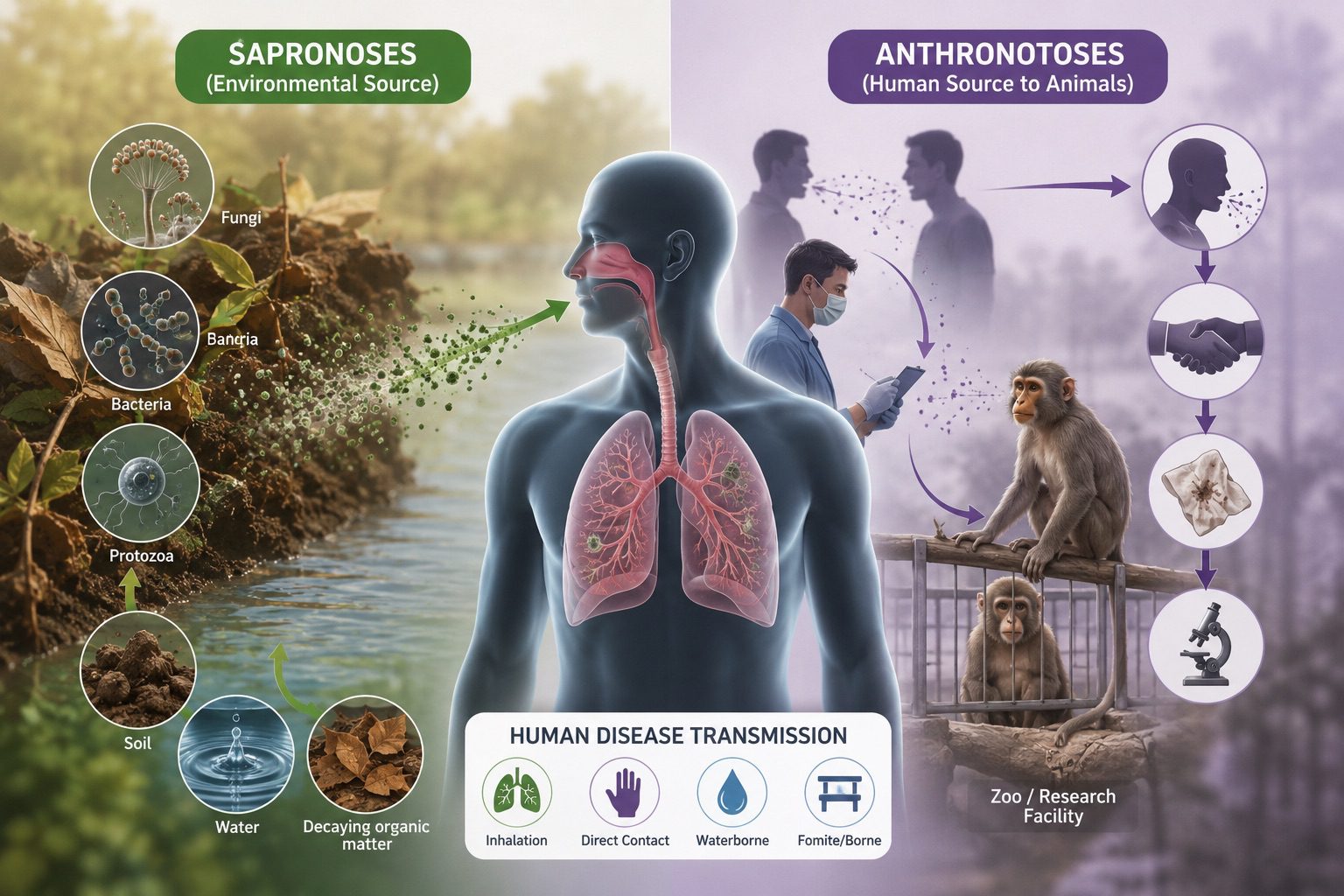
This schematic illustration depicts the contrasting transmission pathways of sapronoses and anthroponoses and their relevance to human disease emergence. On the left, sapronoses originate from abiotic environmental reservoirs such as soil, water, and decaying organic matter, where saprophytic microorganisms including fungi, bacteria, and protozoa can persist and replicate before infecting humans through environmental exposure. On the right, anthroponoses are maintained within human populations and may be transmitted from humans to susceptible animal hosts, particularly non-human primates, through direct contact or respiratory routes. The central human figure highlights the role of humans as a convergence point between environmental and biological transmission systems. Together, these pathways illustrate the complex interactions among humans, animals, and environmental reservoirs that shape infectious disease ecology and public health risks.
Transmission dynamics and evolutionary transitions between zoonotic and anthroponotic systems
The relationship between anthroponotic diseases and zoonoses is fundamentally shaped by transmission dynamics and evolutionary constraints acting on pathogens as they move across species boundaries. Zoonotic pathogens originate in animal reservoirs where they circulate in established ecological cycles involving wildlife, livestock, or synanthropic species. Human infection occurs when ecological disruption, behavioral exposure, or vector activity enables cross-species transmission. However, in most cases, these infections do not immediately establish sustained human-to-human transmission, meaning humans remain epidemiological dead-end hosts. This is a defining feature of many zoonoses and reflects incomplete adaptation to human physiology and transmission networks.
The transition from zoonosis to anthroponosis requires a pathogen to acquire efficient human-to-human transmissibility. This involves evolutionary changes in receptor binding, replication efficiency in human tissues, immune evasion mechanisms, and transmission route optimization (e.g., respiratory, sexual, or fecal-oral pathways). Once these adaptations are achieved, the pathogen no longer relies on animal reservoirs for persistence and becomes fully anthroponotic. This transition is not binary but exists along a continuum, where some pathogens maintain dual circulation in both animals and humans during intermediate stages.
Anthroponotic and zoonotic systems remain linked even after such transitions. Many anthroponotic pathogens retain the ability to infect animal hosts, even if these hosts are not epidemiologically significant for transmission maintenance. This residual cross-species infectivity reflects shared physiological pathways among mammals and other vertebrates. In some cases, reverse zoonosis (anthroponosis to animals) can establish secondary reservoirs, which may later reintroduce genetically similar pathogens into human populations. This feedback loop creates a complex ecological network rather than a linear transmission pathway.
Epidemiologically, zoonoses are often characterized by sporadic human cases or outbreaks triggered by repeated exposure to infected animals, whereas anthroponoses are characterized by sustained epidemic or endemic transmission within human populations. Despite this difference, both systems are governed by similar ecological principles: host density, contact structure, transmission efficiency, and pathogen fitness across different environments. The key distinction lies in where long-term maintenance occurs, not in the absence of cross-species interaction.
From an evolutionary perspective, zoonotic systems serve as reservoirs of genetic diversity for pathogens that may eventually become anthroponotic. Wildlife and domestic animals provide extensive ecological niches where viral recombination, mutation, and reassortment can occur. These processes generate novel variants that may occasionally acquire the capacity for human adaptation. Once introduced into human populations, selective pressures shift toward optimizing human transmission rather than animal persistence, reinforcing the transition toward anthroponosis.
Anthroponotic diseases and zoonoses are not isolated categories but interconnected stages within a broader ecological and evolutionary continuum of infectious disease dynamics. Their linkage is maintained through recurrent spillover events, bidirectional transmission potential, and shared environmental interfaces that facilitate pathogen movement between humans and animals. Understanding this continuum is essential for predicting emerging infectious diseases and designing interventions that target not only human populations but also the animal reservoirs that sustain zoonotic circulation.
Sapronoses: abiotic environmental reservoirs and dual-lifestyle pathogens
Sapronoses represent a distinct ecological category of infectious diseases in which the primary reservoir is not a living host but an abiotic environmental substrate. A defining feature of sapronotic agents is their dual lifestyle. These organisms alternate between a saprophytic phase, in which they exist freely in the environment, and a parasitic phase, in which they infect and cause disease in warm-blooded vertebrates, including humans. In the saprophytic phase, pathogens survive at ambient environmental temperatures, utilizing decaying organic matter as a nutrient source. In the parasitic phase, they must adapt rapidly to the higher and more stable temperatures of homeothermic hosts, typically around 37°C in humans. This thermal transition is a critical biological barrier that distinguishes sapronotic organisms from many other environmental microbes and underpins their pathogenic potential.
Sapronoses are particularly associated with fungi, bacteria, and certain protozoa that possess environmental resilience and metabolic flexibility. Among the most important sapronotic pathogens are dimorphic fungi responsible for systemic or visceral mycoses. These include agents of coccidioidomycosis and histoplasmosis, which can persist in soil enriched with organic material such as bird or bat droppings. In these cases, environmental disturbance such as construction, agriculture, or dust storms can aerosolize infectious particles, leading to inhalational exposure in humans.
Superficial dermatophytes, such as Microsporum gypseum, further illustrate the ecological diversity of sapronotic organisms, as they are commonly found in soil and can infect keratinized tissues following environmental contact. Bacterial sapronoses are exemplified by Legionella pneumophila, which thrives in aquatic environments, particularly in artificial water systems such as cooling towers, plumbing networks, and air-conditioning units. In such settings, the organism can replicate within biofilms and protozoa, enhancing its persistence and infectivity. Protozoan sapronoses, including primary amoebic meningoencephalitis caused by Naegleria fowleri, highlight the capacity of free-living organisms to become lethal opportunistic pathogens when introduced into human hosts through environmental exposure.
A key epidemiological distinction of sapronoses is that intracellular parasites such as viruses, rickettsiae, and chlamydiae are excluded from this category, as they require living host cells for replication and cannot complete their life cycles in abiotic substrates. This reinforces the conceptual importance of sapronoses as diseases of independent environmental replication rather than passive environmental contamination.
From a public health perspective, sapronotic diseases are particularly challenging to control because their reservoirs are diffuse, persistent, and often impossible to eliminate. Unlike anthroponotic infections, which can be interrupted through vaccination or isolation, or zoonotic infections, which may be controlled through animal reservoir management, sapronoses require environmental interventions such as water treatment, dust control, and engineering modifications to reduce exposure risk. Their epidemiology is therefore strongly influenced by climatic conditions, land use changes, and human interaction with natural or artificial ecosystems.
Anthroponoses as human-driven transmission systems and their interface with animal hosts
Although anthroponoses are fundamentally defined by human reservoir maintenance, their interaction with animal populations is ecologically significant. In many cases, anthroponotic transmission to animals occurs through close contact, shared environments, or direct exposure to human bodily fluids or respiratory secretions. Among non-human animals, primates are particularly susceptible to anthroponotic infections due to their close genetic and physiological similarity to humans. This similarity includes comparable immune system structures, receptor compatibility, and cellular pathways that facilitate pathogen entry and replication.
Anthroponotic transmission to animals is especially relevant in captive environments such as zoos, research laboratories, and wildlife rehabilitation centers, where close proximity between humans and animals increases the likelihood of cross-species infection. In these settings, diseases can spread from caretakers or visitors to susceptible animal populations, sometimes leading to outbreaks that mirror human disease dynamics. This phenomenon underscores the permeability of species boundaries in infectious disease ecology and highlights the importance of biosafety measures in human–animal interfaces.
Examples of anthroponotic transmission include infections such as tuberculosis and leishmaniasis, which, while primarily considered zoonotic in many contexts, can also be transmitted from humans to animals under certain conditions. In such cases, humans act as the initiating reservoir, and animals become secondary hosts. The directionality of transmission may therefore shift depending on local epidemiological circumstances, making these diseases ecologically flexible rather than strictly unidirectional.
The mode of transmission in anthroponotic diseases is often dependent on direct physical contact, particularly skin-to-skin exposure, respiratory droplets, or contact with contaminated surfaces. This reflects the central role of human behavior and social interaction in sustaining transmission chains. Because humans serve as the main reservoir, anthroponotic diseases are strongly influenced by population density, mobility patterns, hygiene practices, and healthcare infrastructure. Unlike sapronoses, which are governed by environmental persistence, anthroponotic systems are primarily governed by host-to-host interaction networks.
A critical feature of anthroponotic systems is their capacity to sustain long-term transmission within human populations without requiring external reservoirs. However, their ecological interface with animals introduces additional complexity. Once introduced into animal populations, anthroponotic pathogens may undergo further adaptation, potentially establishing new transmission cycles or reverting back into human populations in altered forms. This bidirectional exchange contributes to the broader evolutionary dynamics of infectious diseases, where host shifts and spillback events can reshape transmission networks.
In terms of prevention and control, anthroponotic diseases in animal populations can often be mitigated through strategies originally developed for human medicine. Vaccination is a particularly important tool in this context, as it can be applied not only to humans but also to susceptible animal species in high-risk environments. For example, primates in captivity may be vaccinated with immunizations similar to those used in humans, reducing the risk of cross-species transmission. This approach reflects a One Health perspective, which recognizes the interconnectedness of human and animal health and the need for integrated disease management strategies.
Clinical relevance and applications of sapronoses and anthroponoses in medicine and public health
Sapronoses and anthroponoses have distinct but complementary clinical and public health relevance because they represent fundamentally different infection sources abiotic environmental reservoirs versus human reservoirs with occasional cross-species transmission. Understanding these categories directly informs diagnostic reasoning, infection control strategies, outbreak investigation, and preventive medicine. In clinical practice, their importance lies not only in identifying causative agents but also in determining exposure pathways, predicting disease patterns, and designing appropriate interventions.
Sapronoses are clinically significant because they often present as sporadic, environmentally acquired infections that are difficult to trace epidemiologically. Since their reservoirs are abiotic soil, water systems, decaying organic matter, or engineered environments patients typically lack identifiable human or animal contact history. This can delay diagnosis, especially when infections mimic more common respiratory, neurological, or systemic diseases. Sapronotic pathogens frequently cause severe disease in humans despite limited human-to-human transmission capacity, reflecting their evolutionary adaptation to environmental rather than host-based survival. Clinically important examples include invasive fungal infections such as histoplasmosis and coccidioidomycosis, opportunistic aspergillosis, and cryptococcal disease, as well as bacterial infections like legionellosis and protozoal infections such as primary amoebic meningoencephalitis.
From a clinical standpoint, sapronoses require a high index of suspicion in patients with relevant environmental exposures, such as soil disruption, construction work, freshwater contact, or exposure to contaminated water systems. Diagnosis often depends on specialized laboratory methods including culture from environmental samples, antigen detection, molecular diagnostics, and imaging patterns suggestive of systemic fungal or atypical bacterial infection. Treatment strategies are frequently prolonged and involve antifungal or antimicrobial therapy that must account for intrinsic environmental resilience and, in some cases, intracellular survival within host macrophages. Importantly, prevention relies heavily on environmental engineering and public health infrastructure, such as water system disinfection, air filtration, and control of aerosol-generating environmental sources rather than patient isolation.
Anthroponoses, in contrast, are clinically relevant because they depend on continuous human-to-human transmission chains. This makes them highly responsive to interventions targeting human behavior, vaccination, and infection control practices. Diseases in this category often present in clusters, outbreaks, or endemic patterns shaped by population density and social interaction. Classic anthroponotic infections include tuberculosis, measles, gonorrhea, and diphtheria. Clinically, these diseases require rapid identification and interruption of transmission through isolation of cases, contact tracing, chemoprophylaxis, and immunization programs where available.
A key clinical advantage in managing anthroponoses is that humans are the primary reservoir, meaning that effective intervention can theoretically eliminate the pathogen from circulation without needing to address environmental or animal reservoirs. This underpins the success of eradication and elimination programs, such as the global eradication of smallpox and substantial reduction of vaccine-preventable diseases. However, anthroponotic diseases also pose significant challenges in healthcare settings, where nosocomial transmission can occur rapidly if infection control measures are inadequate. This makes hospital hygiene, screening protocols, and vaccination coverage critical components of clinical practice.
Both sapronoses and anthroponoses are increasingly relevant in the context of emerging infectious diseases and antimicrobial resistance. Sapronotic organisms can serve as environmental reservoirs for resistant genes, while anthroponotic pathogens facilitate rapid dissemination of resistant strains through dense human networks. In addition, climate change, urbanization, and environmental disruption are expanding the range of sapronotic exposures, while globalization and mobility intensify anthroponotic transmission dynamics.
In applied clinical and public health contexts, integrating knowledge of both categories supports a One Health approach, which recognizes that human disease is shaped by environmental conditions, microbial ecology, and population-level interactions. This integrated perspective improves outbreak preparedness, enhances diagnostic accuracy, and guides targeted interventions that address both immediate clinical management and long-term disease prevention strategies.
Saprozoonoses: infectious diseases sustained through interactions between animal hosts and environmental reservoirs
A saprozoonosis is an infectious disease caused by a pathogen that requires both a vertebrate animal host and an abiotic environmental reservoir for its maintenance, development, or transmission in nature. Unlike pathogens that are maintained exclusively in humans or solely within environmental substrates, saprozoonotic agents depend on a combination of biological and environmental components to complete their life cycle. In these diseases, animals serve as essential hosts that harbor, amplify, or shed the pathogen, while environmental media such as soil, water, sediments, or vegetation provide conditions necessary for the pathogen’s survival, maturation, or infective development. The pathogen cannot be maintained indefinitely through animal hosts alone or through the environment alone; rather, both components are required for successful transmission and persistence.
Humans are typically incidental hosts who become infected through contact with contaminated environmental sources, infected animals, or infective stages that have developed outside the host. The epidemiology of saprozoonoses is therefore influenced by environmental conditions, animal population dynamics, land-use practices, climate variability, and human behavior. Because these diseases involve complex interactions among animals, humans, and environmental reservoirs, they are of particular importance within the One Health framework. Effective prevention and control often require integrated approaches that address animal health, environmental management, and human exposure pathways simultaneously.
Examples of saprozoonotic diseases include: Toxocariasis, in which eggs shed by dogs and cats develop into infective stages in soil before infecting humans; Fascioliasis, where transmission involves livestock, freshwater environments, and aquatic vegetation; and Paragonimiasis, which requires animal hosts and environmental aquatic stages. Other examples include Echinococcosis and Ascariasis in animal-associated transmission cycles where infective stages develop in the environment before infecting new hosts.
How saprozoonoses differ from anthroponoses and sapronoses.
Saprozoonoses differ from anthroponoses because anthroponotic diseases are maintained primarily through human-to-human transmission, with humans serving as the principal reservoir and source of infection. They differ from sapronoses because sapronotic pathogens can survive and often multiply independently in abiotic environments without requiring animal hosts for their persistence. In contrast, saprozoonotic pathogens rely on a dual reservoir system involving both vertebrate animals and environmental substrates. Consequently, anthroponoses are sustained mainly by human populations, sapronoses by environmental reservoirs, whereas saprozoonoses require the combined participation of animal hosts and environmental stages to maintain their natural transmission cycle and long-term ecological persistence.
References
Lederberg J. Infectious disease as an evolutionary paradigm. Emerg Infect Dis. 1997;3:417–23.
Bell JC, Palmer SR, Payne JM. The zoonoses (infections transmitted from animals to man). London: Arnold; 1988.
World Health Organization. Joint WHO/FAO expert committee on zoonoses. 2nd report. WHO technical report series no. 169, Geneva; 1959. 3rd report, WHO Technical Report Series no. 378, Geneva; The Organization; 1967.
Pavlovsky EN. Natural nidality of transmissible diseases. Urbana (IL): University of Illinois Press; 1966.
Beaty BJ, Marquardt WC, eds. The biology of disease vectors. Niwot (CO): University Press of Colorado; 1996.
Terskikh VI. Diseases of humans and animals caused by microbes able to reproduce in an abiotic environment that represents their living habitat [in Russian]. Zhurn Mikrobiol Epidemiol Immunobiol (Moscow). 1958;8:118–22.
Somov GP, Litvin VJ. Saprophytism and parasitism of pathogenic bacteria—ecological aspects (in Russian). Novosibirsk: Nauka; 1988.
Krauss H, Weber A, Enders B, Schiefer HG, Slenczka W, Zahner H. Zoonosen, 2. Aufl. Köln: Deutscher Ärzte-Verlag; 1997.
Schwabe CV. Veterinary medicine and human health. Baltimore: Williams & Wilkins; 1964.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.


