The Parvoviridae family comprises a group of very small DNA viruses that infect both humans and animals. Members of this family are among the smallest known pathogenic viruses and are characterized by their simple structure and dependence on actively dividing host cells for replication. The Parvoviridae family contains important viruses capable of infecting both humans and animals. The human parvovirus B19 represents the most clinically significant member of the Parvoviridae family. Although infection is often mild in healthy individuals, severe complications can occur in pregnant women, immunocompromised patients, and individuals with underlying haematological disorders.
Historically, the Parvoviridae family was classified into six genera:
- Parvovirus,
- Contravirus,
- Erythrovirus,
- Dependovirus,
- Densovirus, and
- Iteravirus.
Among these, human parvovirus B19, classified under the genus Erythrovirus in older classifications, is the most medically significant because it causes disease in humans.
Parvoviruses are widely distributed throughout the world and can infect a variety of vertebrate and invertebrate hosts. Human infections occur globally and are particularly common during childhood. Although many infections are mild or asymptomatic, some can lead to severe complications in vulnerable populations.
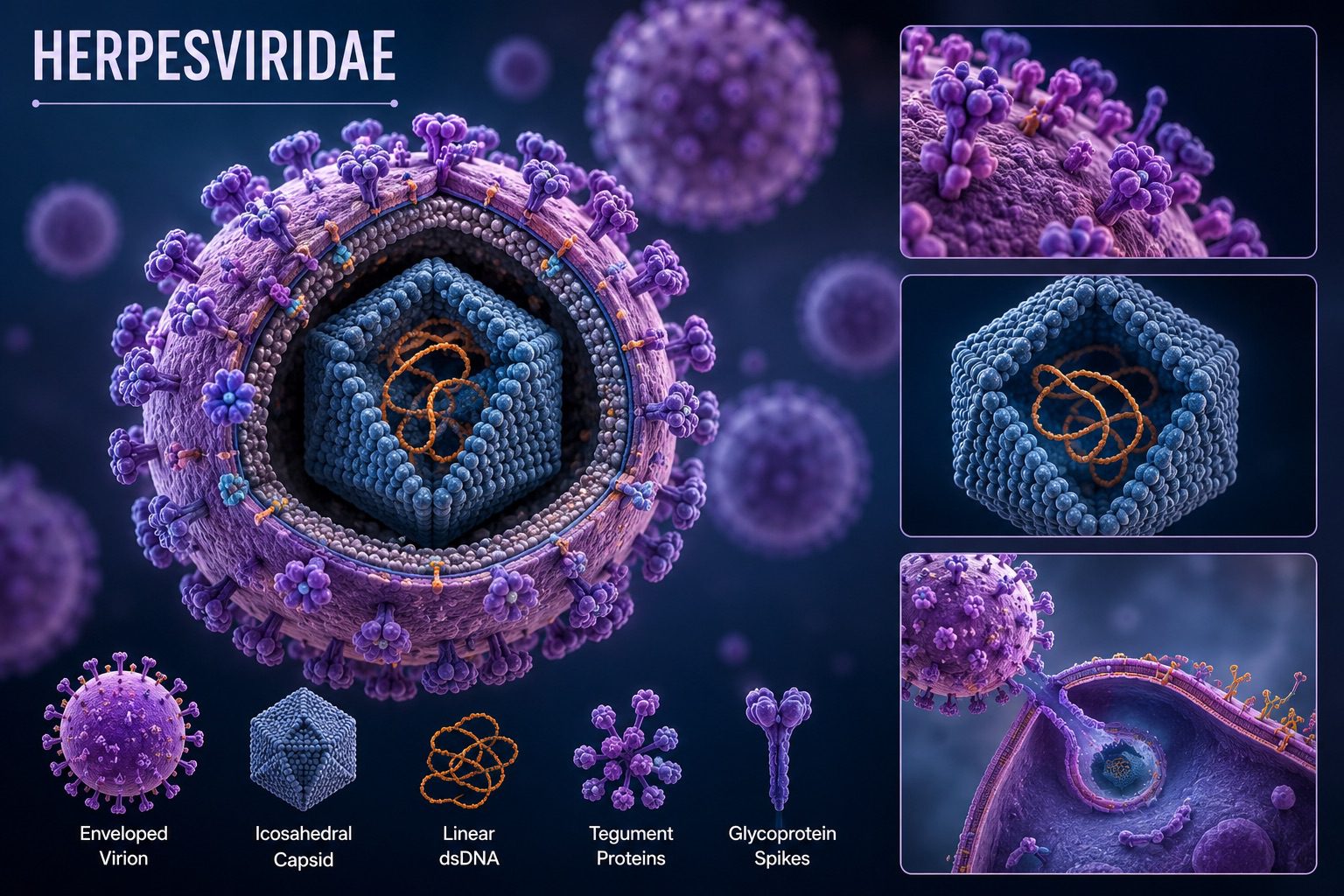
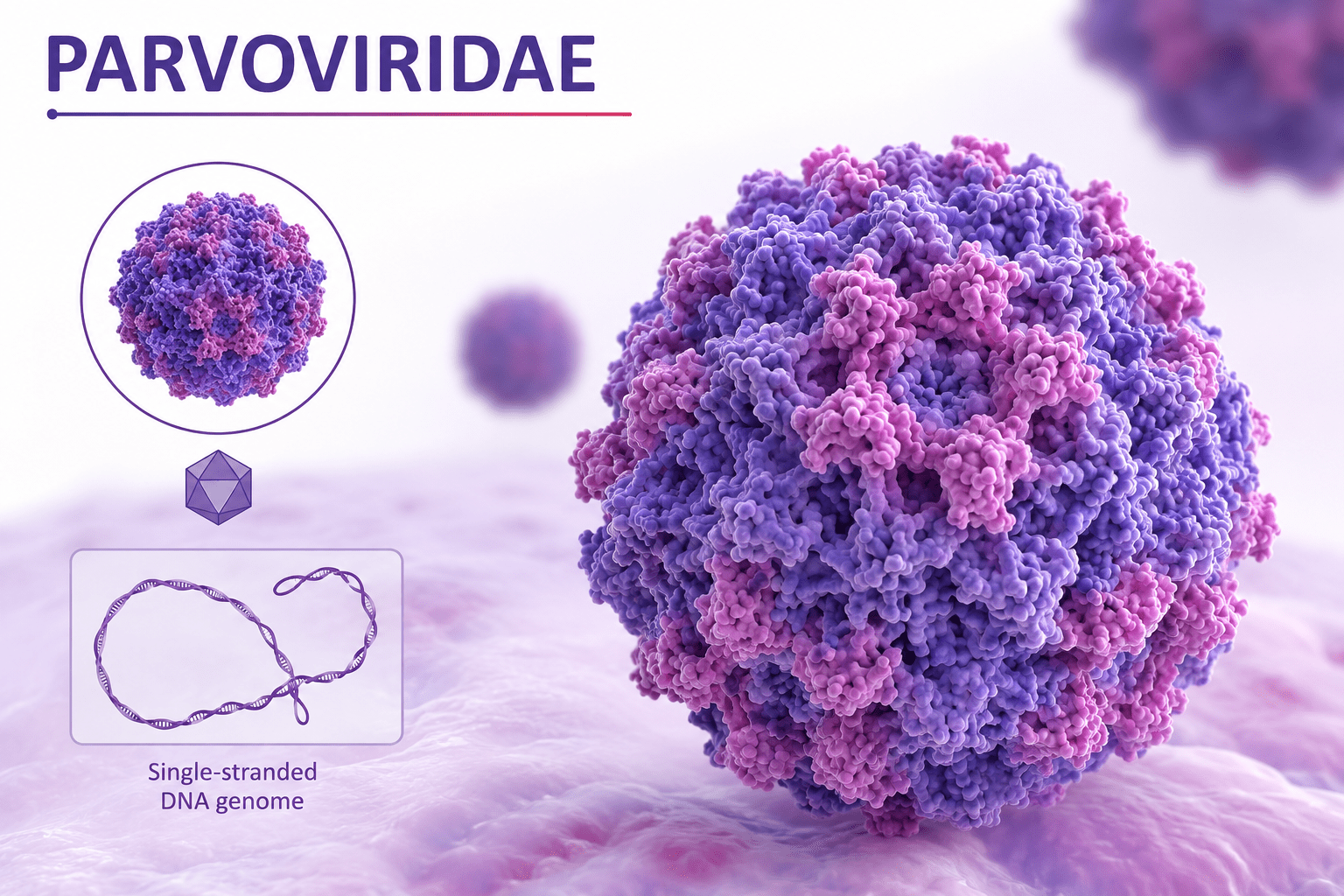
Structurally, viruses in the Parvoviridae family are small, non-enveloped (naked) viruses measuring approximately 18-26 nm in diameter. They possess an icosahedral capsid that encloses a linear single-stranded DNA (ssDNA) genome. Because these viruses lack a lipid envelope, they are generally more resistant to environmental stress than enveloped viruses.
The absence of an envelope contributes to several important biological characteristics of the Parvoviridae family as follows:
- Resistance to ether and lipid solvents
- Relative stability at elevated temperatures
- Ability to persist in the environment for longer periods
- Release from infected cells primarily through cell lysis
Despite this environmental resilience, parvoviruses are susceptible to inactivation by chlorine-containing disinfectants, formalin, and ultraviolet (UV) radiation.
Replication of parvoviruses occurs within the nucleus of infected host cells. Since these viruses possess a limited genetic capacity, they rely heavily on host cellular machinery for viral DNA replication and protein synthesis. Successful replication generally requires actively dividing cells because host DNA polymerases needed for viral genome replication are abundant during cellular division.
Human parvovirus B19 demonstrates a marked preference for infecting erythroid precursor cells located in the bone marrow, which are responsible for producing red blood cells (erythrocytes). This cellular tropism explains many of the clinical manifestations associated with infection.
Human Parvovirus B19: Pathogenesis and Clinical Manifestations
Human parvovirus B19 is the most clinically important human pathogen within the Parvoviridae family and is responsible for a wide spectrum of diseases ranging from mild childhood illness to severe haematological and fetal complications. The outcome of infection depends largely on several host factors including age, immune status, pregnancy status, and the presence of underlying blood disorders. While infection is often self-limiting in healthy individuals, it can produce serious disease in vulnerable populations.
Human parvovirus B19 exhibits a strong tropism for erythroid precursor cells, which are immature red blood cell-producing cells found primarily in the bone marrow. The virus enters these cells through specific cellular receptors and replicates within their nuclei. Viral replication eventually destroys the infected cells, interrupting normal red blood cell production. This mechanism forms the basis for many of the clinical manifestations associated with infection.
One of the most common diseases caused by human parvovirus B19 is erythema infectiosum, commonly referred to as fifth disease. Fifth disease is predominantly a childhood infection and is classified among the traditional childhood exanthematous illnesses characterized by fever and skin eruptions. The disease occurs worldwide and is especially common among school-aged children because of frequent close contact and efficient respiratory transmission.
Following exposure to the virus, the incubation period usually ranges from 12-18 days, although slight variations may occur among individuals. During the early stage of infection, symptoms are generally mild and nonspecific, making diagnosis difficult before the appearance of the characteristic rash.
Common early manifestations of human parvovirus B19 infection include:
- Low-grade fever
- General malaise
- Fatigue or weakness
- Mild upper respiratory tract symptoms
- Headache
- Muscle aches in some cases
These prodromal symptoms often resemble those of a mild viral respiratory infection and may last for several days. As the immune response develops, more recognizable clinical features begin to appear.
The hallmark manifestation of erythema infectiosum is the appearance of a distinctive erythematous facial rash known as “slapped cheek syndrome.” This rash produces a bright red discoloration over both cheeks, creating the impression that the child has been struck across the face. The area around the mouth typically remains pale, creating a characteristic appearance useful for clinical diagnosis.
After the facial rash develops, many children subsequently develop a secondary maculopapular rash involving the trunk, arms, buttocks, and lower limbs. The rash may evolve into a lacy or reticular pattern and can fluctuate in intensity for several weeks. Exposure to heat, exercise, emotional stress, or sunlight may temporarily intensify the rash even after the acute infection has resolved.
In otherwise healthy children, the illness is generally mild and self-limiting, and complete recovery usually occurs without long-term consequences. Once infected, individuals typically develop immunity that protects against future infection. Although many infections remain uncomplicated, human parvovirus B19 becomes clinically significant in individuals with disorders affecting red blood cell production or survival.
A central feature of parvovirus B19 pathogenesis is its ability to infect and destroy erythroid precursor cells in the bone marrow, temporarily suppressing erythropoiesis, the physiological process responsible for generating red blood cells. In healthy individuals, red blood cells normally survive for approximately 120 days; therefore, a temporary reduction in production often produces minimal symptoms.
However, in patients with conditions associated with accelerated red blood cell destruction, the interruption of erythropoiesis may have severe consequences. Individuals at particular risk of infection with Human Parvovirus B19 include those with:
- Sickle cell disease
- Chronic haemolytic anaemia
- Hereditary spherocytosis
- Thalassaemia
- Other disorders requiring continuous red blood cell replacement
In these patients, parvovirus infection may precipitate transient aplastic crisis, a serious condition characterized by sudden failure of red blood cell production. During aplastic crisis:
- Bone marrow production of erythrocytes decreases markedly.
- Existing red blood cells continue undergoing destruction.
- Haemoglobin concentration declines rapidly.
- Severe anaemia develops over a short period.
- Symptoms such as weakness, pallor, dizziness, and shortness of breath may occur.
- Hospitalization and blood transfusion may become necessary.
Although transient aplastic crisis is usually reversible once viral replication ceases, prompt recognition and supportive management are essential. Human parvovirus B19 also presents important challenges in immunocompromised individuals, including patients receiving chemotherapy, transplant recipients, and individuals with impaired immune function. Because viral clearance depends on effective antibody production, these patients may be unable to eliminate the infection completely.
Persistent infection with human parvovirus B19 can lead to:
- Chronic suppression of red blood cell production
- Persistent anaemia
- Continuous viral replication
- Long-term dependence on supportive therapy
Some immunocompromised patients may require treatment with intravenous immunoglobulin (IVIG) to facilitate viral clearance. Another significant manifestation of parvovirus B19 infection occurs in adults, particularly women, where infection may present with arthralgia (joint pain) or arthritis-like symptoms. Joint involvement commonly affects the hands, wrists, knees, and ankles. These symptoms may persist for weeks or occasionally months but generally resolve without permanent joint damage.
Parvovirus B19 infection has particular clinical significance during pregnancy. Maternal infection may result in transplacental transmission, allowing the virus to infect fetal erythroid cells. Since the developing fetus relies heavily on rapid red blood cell production, fetal infection can have severe outcomes.
Complications associated with maternal infection with human parvovirus B19 include:
- Severe fetal anaemia
- Non-immune hydrops fetalis
- Congestive fetal heart failure
- Spontaneous abortion
- Intrauterine fetal death
The risk and severity of complications depend partly on the gestational age at which infection occurs, with infection during the second trimester often receiving particular clinical attention. Despite these potential complications, most maternal infections do not result in fetal loss, and careful obstetric monitoring can improve outcomes.
Although human parvovirus B19 infection may occur at any age, children remain the most commonly affected population, largely because transmission frequently occurs in schools, daycare centres, and households through close interpersonal contact. Understanding the pathogenesis and clinical manifestations of parvovirus B19 remains essential for accurate diagnosis, early recognition of complications, and appropriate patient management across different population groups.
Transmission, epidemiology, diagnosis, treatment, and prevention of human parvovirus B19 infection
Human parvovirus B19 infection occurs worldwide and has no marked geographic restriction, making it a globally distributed viral disease. Infection affects individuals of all age groups, although children remain the most commonly infected population. Community outbreaks frequently occur in environments where close interpersonal contact promotes viral spread, particularly in schools, daycare centres, households, healthcare facilities, and other institutional settings. Seasonal increases in infection may occur in some regions, especially where respiratory infections become more common.
Human parvovirus B19 is highly transmissible, and infected individuals may spread the virus before characteristic symptoms become apparent. This ability to transmit infection during the early phase contributes significantly to unnoticed circulation within communities.
Transmission occurs mainly through three principal routes:
- Respiratory transmission: This is the most common mode of spread and occurs through exposure to respiratory droplets released during coughing, sneezing, or close contact with infected individuals. Transmission is particularly efficient in crowded environments.
- Blood-borne transmission: Infection may occur through exposure to contaminated blood products, blood transfusion, organ transplantation, or accidental exposure to infected blood.
- Vertical (maternal-fetal) transmission: Pregnant women infected with parvovirus B19 may transmit the virus across the placenta to the developing fetus, potentially resulting in adverse fetal outcomes.
The virus is generally most contagious during the prodromal phase, before the appearance of the typical rash. Consequently, many infected individuals unknowingly transmit infection before clinical recognition. Although many infections are mild or asymptomatic, certain populations are at increased risk of developing severe disease or complications. At risk population include:
- Children
- Pregnant women
- Immunocompromised individuals
- Patients with haemolytic disorders
- Individuals with sickle cell disease
- Patients with chronic anaemia
- Individuals with impaired bone marrow function
Children usually develop the classic rash-associated illness known as erythema infectiosum, whereas adults may present with joint pain or more atypical manifestations.
Diagnosis of human parvovirus B19 infection
Diagnosis of parvovirus B19 infection relies on a combination of clinical evaluation and laboratory investigations. Clinical diagnosis may be straightforward in children presenting with the characteristic “slapped-cheek” facial rash followed by a lacy rash over the body. However, laboratory confirmation becomes particularly important in atypical cases, pregnancy, severe anaemia, or immunocompromised patients.
Laboratory diagnostic approaches include:
- Detection of parvovirus B19-specific IgM antibodies, which indicates recent or acute infection.
- Detection of IgG antibodies, suggesting previous exposure and the development of immunity.
- Polymerase chain reaction (PCR) testing to detect viral DNA in blood or tissue samples. PCR is especially useful for immunocompromised individuals, chronic infections, and prenatal investigations.
- In selected cases, haematological assessment may reveal decreased reticulocyte counts and evidence of suppressed red blood cell production.
Therapy for human parvovirus B19 infection
Currently, no specific antiviral therapy has been approved for routine treatment of human parvovirus B19 infection. As a result, treatment is largely supportive and tailored according to disease severity and patient risk factors.
Management strategies may include:
- Rest and adequate hydration for uncomplicated infections
- Antipyretic and analgesic medications for fever, discomfort, and joint symptoms
- Blood transfusion in patients with severe anaemia or transient aplastic crisis
- Intravenous immunoglobulin (IVIG) for selected immunocompromised patients with persistent infection and chronic anaemia
Most healthy individuals recover completely without medical intervention. At present, there is no licensed vaccine or specific prophylactic agent available for prevention of human parvovirus B19 infection. Consequently, prevention and public health control depend primarily on reducing transmission and protecting susceptible populations.
Important preventive and control measures for human parvovirus B19 infection include:
- Frequent hand washing and maintenance of good personal hygiene
- Proper respiratory etiquette, including covering the mouth and nose during coughing or sneezing
- Avoidance of close contact with infected individuals during outbreaks
- Routine infection-control practices in healthcare settings
- Monitoring and follow-up of pregnant women after confirmed exposure
- Careful screening and management of high-risk patients, particularly those with blood disorders or compromised immunity
Early recognition of infection, timely supportive care, and implementation of preventive measures remain essential for reducing disease burden and preventing serious complications associated with human parvovirus B19 infection.
References
Acheson N.H (2011). Fundamentals of Molecular Virology. Second edition. John Wiley and Sons Limited, West Sussex, United Kingdom.
Alan J. Cann (2005). Principles of Molecular Virology. 4th edition. Elsevier Academic Press, Burlington, MA, USA.
Alberts B, Bray D, Johnson A, Lewis J, Raff M, Roberts K and Walter P (1998). Essential Cell Biology: An Introduction to the Molecular Biology of the Cell. Third edition. Garland Publishing Inc., New York.
Barrett J.T (1998). Microbiology and Immunology Concepts. Philadelphia, PA: Lippincott-Raven Publishers. USA.
Black, J.G. (2008). Microbiology: Principles and Explorations (7th ed.). Hoboken, NJ: J. Wiley & Sons.
Brian W.J Mahy and Mark H.C van Regenmortel (2010). Desk Encyclopedia of Human and Medical Virology. Elsevier Academic Press, San Diego, USA.
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA.
Cann A.J (2011). Principles of Molecular Virology. Fifth edition. Academic Press, San Diego, United States.
Carter J and Saunders V (2013). Virology: Principles and Applications. Second edition. Wiley-Blackwell, New Jersey, United States.
Champoux J.J, Neidhardt F.C, Drew W.L and Plorde J.J (2004). Sherris Medical Microbiology: An Introduction to Infectious Diseases. 4th edition. McGraw Hill Companies Inc, USA.
Dimmock N (2015). Introduction to Modern Virology. Seventh edition. Wiley-Blackwell, New Jersey, United States.
Dimmock N.J, Easton A.J and Leppard K.N (2001). Introduction to modern virology. 5th edition. Blackwell Science publishers. Oxford, UK.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.