The family Herpesviridae comprises a large and diverse group of enveloped double-stranded DNA viruses that infect a wide range of vertebrate hosts, including humans and animals. Members of this family are characterized by their ability to establish lifelong latent infections within the host after primary exposure, with periodic reactivation under conditions such as stress, immunosuppression, or disease. Due to their persistent nature and broad clinical significance, herpesviruses are among the most extensively studied viral pathogens in medical and veterinary virology.
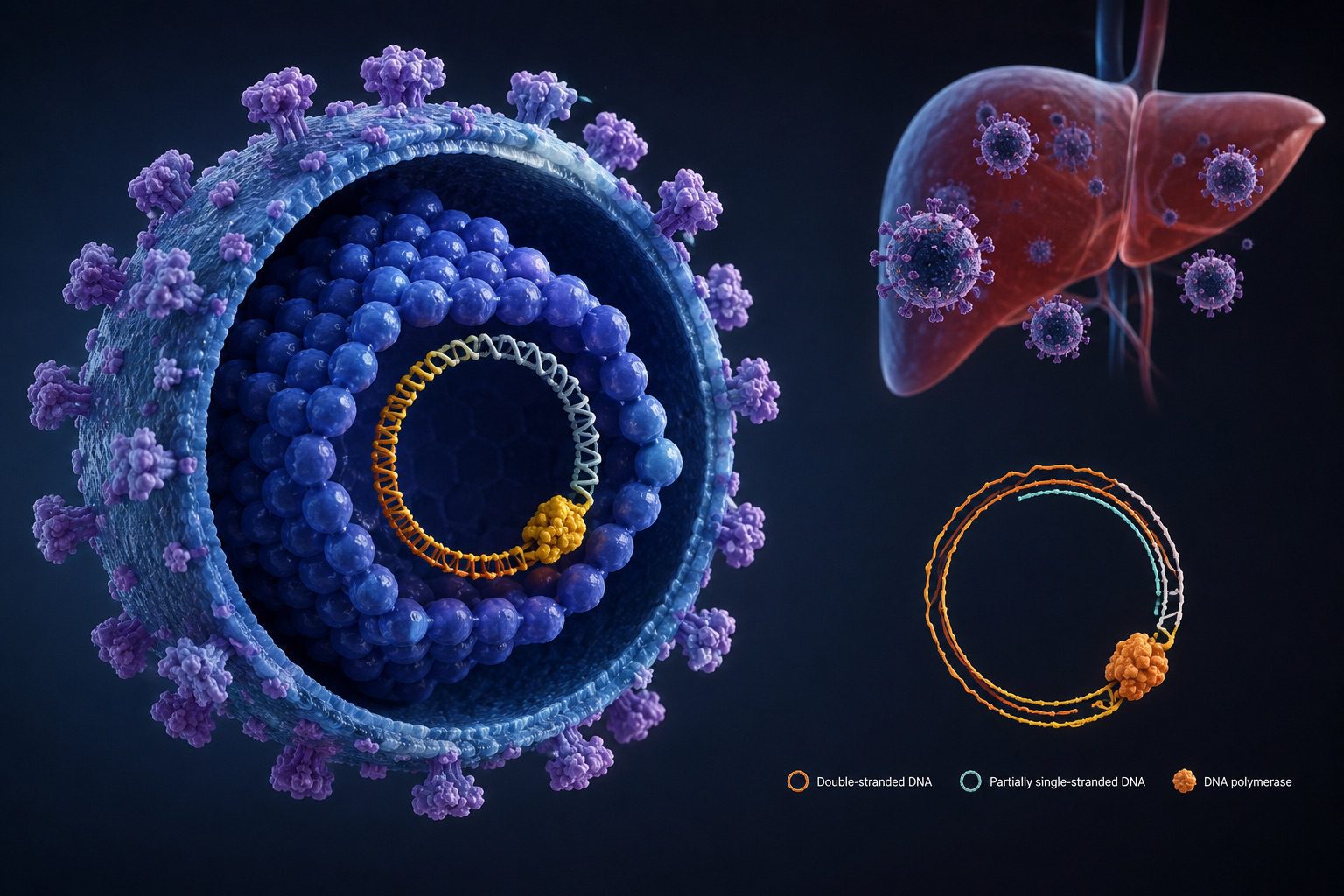
Structurally, herpesviruses possess a linear double-stranded DNA genome enclosed within an icosahedral capsid, surrounded by a proteinaceous tegument layer and a lipid envelope containing viral glycoproteins essential for host-cell attachment and entry. The viral genome is relatively large, ranging from approximately 120 to 240 kilobase pairs, allowing these viruses to encode numerous proteins involved in replication, immune evasion, and latency. Replication typically occurs within the nucleus of infected cells, where viral DNA synthesis and capsid assembly take place.
The family Herpesviridae is taxonomically divided into three major subfamilies based on biological properties, tissue tropism, and replication characteristics: Alphaherpesvirinae, Betaherpesvirinae, and Gammaherpesvirinae. Alphaherpesviruses, such as herpes simplex virus type 1 (HSV-1), herpes simplex virus type 2 (HSV-2), and varicella-zoster virus (VZV), are characterized by rapid replication and latency in sensory ganglia. Betaherpesviruses, including cytomegalovirus (CMV) and human herpesvirus 6 (HHV-6), replicate more slowly and establish latency in secretory glands, lymphoreticular cells, and kidneys. Gammaherpesviruses, such as Epstein-Barr virus (EBV) and Kaposi’s sarcoma-associated herpesvirus (KSHV), primarily infect lymphoid tissues and are associated with several malignancies.
Human herpesviruses are responsible for a wide spectrum of diseases ranging from mild mucocutaneous lesions to severe systemic infections and cancers, particularly in immunocompromised individuals. Beyond human health, herpesviruses also cause economically significant diseases in livestock, poultry, and companion animals. Their ability to evade host immune responses, establish latency, and reactivate periodically presents major challenges for disease control and therapeutic intervention. Consequently, ongoing research on the molecular biology, pathogenesis, epidemiology, and antiviral resistance of herpesviruses remains essential for the development of effective vaccines, diagnostics, and treatment strategies.
Structure of the Herpesviridae family
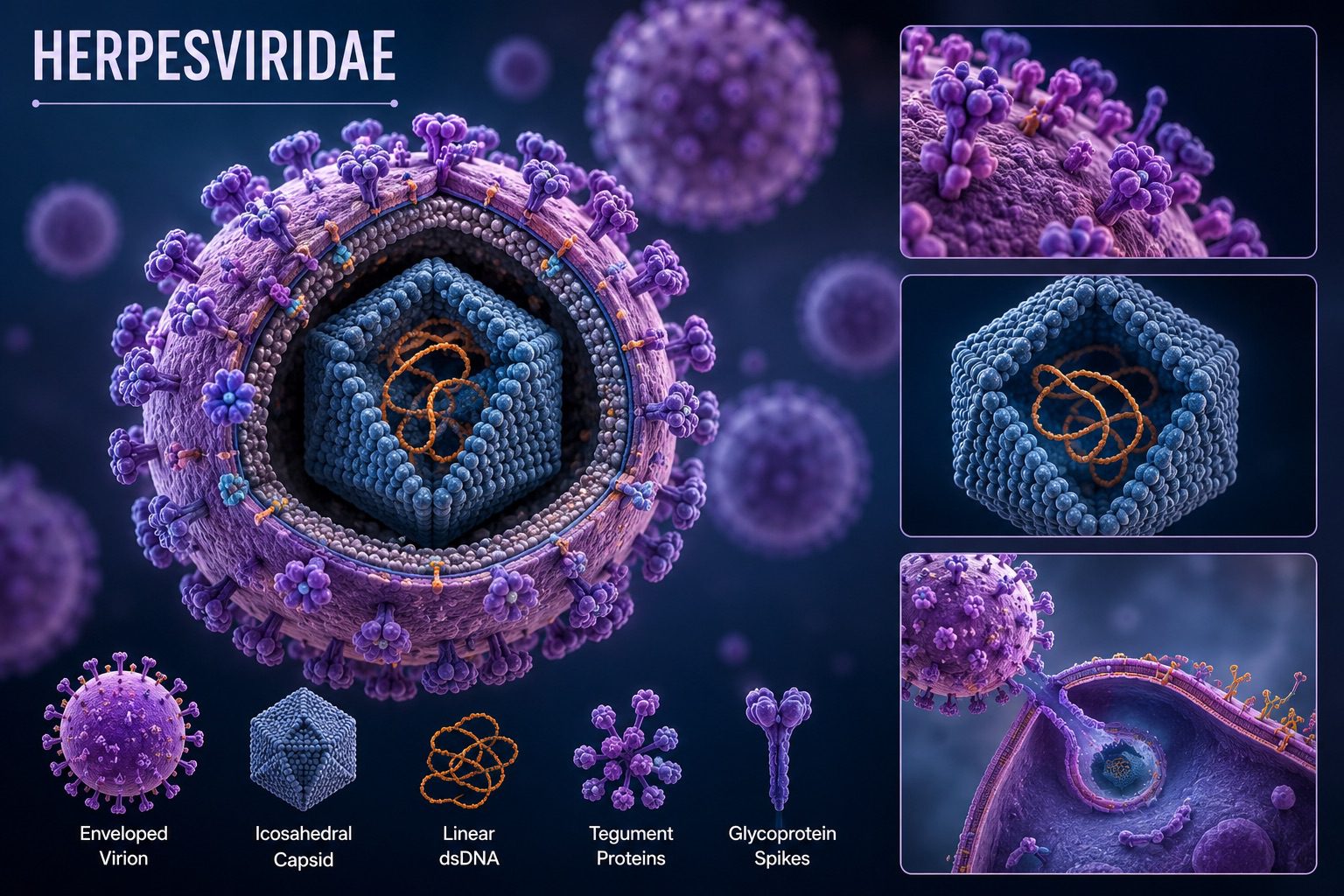
Members of the Herpesviridae family possess a complex and highly organized virion structure that contributes significantly to their infectivity, persistence, and pathogenicity. Herpesviruses are among the largest animal viruses, with virion diameters ranging from approximately 120 to 300 nm. Despite variation among species, all herpesviruses share a common structural architecture consisting of four principal components: the core, capsid, tegument, and envelope.
At the center of the virion lies the viral core, which contains a linear double-stranded DNA (dsDNA) genome. The genome size varies between approximately 120 and 240 kilobase pairs depending on the virus species, allowing herpesviruses to encode more than 70 to 200 proteins involved in replication, host interaction, immune evasion, and latency. The viral DNA is densely packed within the capsid in a toroidal arrangement, ensuring stability and protection of the genetic material during transmission between host cells.
Surrounding the core is the icosahedral capsid, a highly symmetrical protein shell composed mainly of capsomeres formed from viral structural proteins (Figure 1). The capsid typically exhibits T=16 icosahedral symmetry and measures approximately 100-110 nm in diameter. Its primary function is to protect the viral genome from environmental degradation and facilitate delivery of the DNA into the host cell nucleus during infection. The capsid is constructed from several viral proteins, with the major capsid protein forming the bulk of the shell and smaller accessory proteins stabilizing the structure. A specialized portal complex located at one vertex of the capsid allows entry and exit of viral DNA during packaging and infection.
Between the capsid and the envelope is an amorphous protein layer known as the tegument. This unique feature distinguishes herpesviruses from many other enveloped viruses. The tegument contains numerous viral proteins, enzymes, regulatory molecules, and messenger RNAs that are released into the host cell immediately after viral entry. Tegument proteins play crucial roles in initiating viral replication, modulating host immune responses, altering cellular metabolism, and facilitating transport of the capsid toward the nucleus. Some tegument proteins also interfere with host antiviral defenses, thereby enhancing viral survival and persistence.

The outermost layer of the virion is the lipid envelope, which is derived from host cellular membranes during viral budding. Embedded within this envelope are several viral glycoproteins arranged as spikes on the virion surface. These glycoproteins are essential for attachment to host cell receptors, membrane fusion, and entry into susceptible cells. Important glycoproteins such as gB, gC, gD, and gH/gL complexes mediate host-cell recognition and penetration. Because these surface proteins are exposed to the host immune system, they are major targets for neutralizing antibodies and vaccine development.
The structural organization of herpesviruses is closely associated with their biological behavior. The envelope facilitates efficient cell entry but also makes the virus susceptible to detergents, heat, and lipid solvents. In contrast, the stable capsid and tegument support intracellular transport and establishment of latent infections. This sophisticated virion structure enables herpesviruses to replicate efficiently, evade host immunity, and persist lifelong within infected hosts.
Host range of the Herpesviridae family
The Herpesviridae family exhibits a broad but highly species-specific host range, infecting a wide variety of vertebrate animals including humans, mammals, birds, reptiles, amphibians, and fish. Although herpesviruses are widely distributed among animal populations, most members of the family are adapted to a particular host species and rarely infect unrelated hosts under natural conditions. This strong host specificity results from long-term co-evolution between the virus and its host, enabling efficient replication, latency, and immune evasion.
In humans, nine recognized herpesviruses have been identified, including herpes simplex viruses (HSV-1 and HSV-2), varicella-zoster virus (VZV), Epstein-Barr virus (EBV), cytomegalovirus (CMV), and Kaposi’s sarcoma-associated herpesvirus (KSHV). Each virus demonstrates preference for specific tissues or cell types, a phenomenon known as tissue tropism. For example, alphaherpesviruses commonly infect epithelial cells and establish latency in sensory neurons, whereas gammaherpesviruses primarily target lymphocytes.
Animal herpesviruses are also of major veterinary importance. Examples include bovine herpesvirus in cattle, equine herpesvirus in horses, Marek’s disease virus in poultry, and feline herpesvirus in cats. These viruses cause respiratory, neurological, reproductive, and neoplastic diseases, leading to significant economic losses in animal production systems worldwide.
Pathogenesis of the Herpesviridae family
The pathogenesis of viruses belonging to the Herpesviridae family is characterized by a complex interaction between viral replication, immune evasion, latency, and reactivation within the host. A defining feature of all herpesviruses is their ability to establish lifelong latent infections after primary exposure, allowing the virus to persist in the host for extended periods and reactivate intermittently. This biological property contributes significantly to the widespread prevalence and clinical importance of herpesvirus infections in humans and animals.
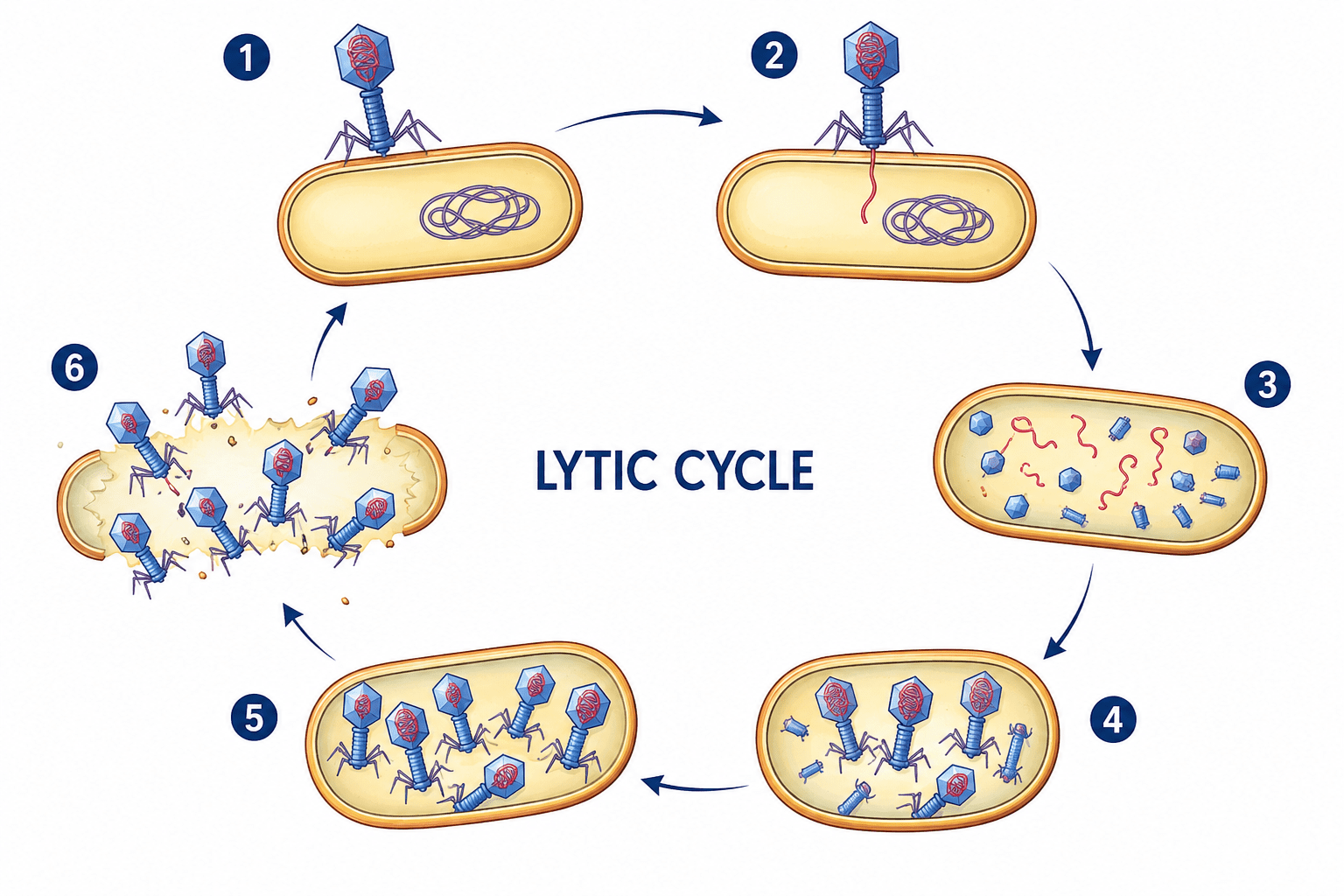
Infection typically begins when viral particles come into contact with susceptible mucosal surfaces, epithelial tissues, or damaged skin. Viral glycoproteins present on the envelope mediate attachment to specific host-cell receptors, facilitating fusion of the viral envelope with the host-cell membrane. Once entry occurs, the nucleocapsid is transported to the nucleus, where the viral DNA is released and replication is initiated. During the lytic phase of infection, viral genes are expressed in a coordinated sequence involving immediate-early, early, and late genes. Immediate-early genes regulate viral replication and host-cell modulation, early genes are mainly involved in DNA synthesis, while late genes encode structural proteins necessary for virion assembly.
Primary replication commonly occurs in epithelial cells at the site of entry, resulting in local tissue damage and inflammatory responses. Cell destruction occurs due to viral cytopathic effects, including cell lysis, syncytium formation, and intranuclear inclusion body formation. Clinical manifestations such as vesicular lesions, ulcers, fever, and inflammation arise from both direct viral damage and the host immune response. In some herpesvirus infections, the virus may spread locally through cell-to-cell transmission, which allows evasion of circulating antibodies.
Following primary replication, herpesviruses invade specific target cells where latency is established. The site of latency differs among herpesvirus subfamilies. Alphaherpesviruses, such as herpes simplex virus (HSV) and varicella-zoster virus (VZV), establish latency primarily in sensory neurons of peripheral ganglia. Betaherpesviruses, including cytomegalovirus (CMV), persist in monocytes, macrophages, and glandular tissues, whereas gammaherpesviruses such as Epstein-Barr virus (EBV) establish latency mainly in B lymphocytes. During latency, the viral genome persists in host cells as an episomal circular DNA molecule with minimal gene expression and no production of infectious virions. This dormant state allows the virus to escape immune detection and remain within the host indefinitely.
Reactivation of latent herpesviruses may occur due to physiological stress, fever, ultraviolet radiation, hormonal changes, immunosuppression, or concurrent infections. Reactivation results in renewed viral replication and transport of virions back to peripheral tissues, causing recurrent disease manifestations. In HSV infections, reactivation often leads to recurrent oral or genital lesions, while reactivation of VZV causes herpes zoster (shingles). In immunocompromised individuals, reactivation can result in severe systemic disease affecting the lungs, liver, brain, or eyes.
An important aspect of herpesvirus pathogenesis is immune evasion. Herpesviruses have evolved multiple mechanisms to avoid host immune defenses and ensure long-term persistence. These mechanisms include inhibition of antigen presentation through downregulation of major histocompatibility complex (MHC) molecules, interference with cytokine signaling pathways, suppression of apoptosis, and production of viral homologs of immune regulatory proteins. Some herpesviruses also inhibit interferon responses and natural killer (NK) cell activity, reducing the efficiency of innate immunity. Such strategies allow the virus to replicate while minimizing immune-mediated clearance.
In addition to acute infections, certain herpesviruses are associated with oncogenesis and chronic disease. EBV has been linked to Burkitt lymphoma, nasopharyngeal carcinoma, and Hodgkin lymphoma, while Kaposi’s sarcoma-associated herpesvirus is associated with Kaposi’s sarcoma and primary effusion lymphoma. Viral oncogenesis occurs through expression of latent viral proteins that alter cell-cycle regulation, inhibit apoptosis, and promote uncontrolled cellular proliferation.
Host immune status plays a major role in determining disease severity and outcome. In immunocompetent individuals, herpesvirus infections are often mild or self-limiting, whereas neonates, transplant recipients, and individuals with immunodeficiency may develop severe disseminated infections. Persistent inflammation and repeated viral reactivation can also contribute to tissue damage and long-term complications.
Detection of Herpesviridae infections
Accurate detection of viruses belonging to the Herpesviridae family is essential for effective clinical management, epidemiological surveillance, and prevention of disease transmission. Because herpesviruses establish latent infections and may reactivate intermittently, diagnosis often requires a combination of clinical evaluation and laboratory-based techniques. Diagnostic methods vary depending on the virus involved, the stage of infection, and the type of clinical specimen available.
Traditional diagnostic approaches include viral isolation through cell culture. In this method, clinical samples such as vesicular fluid, blood, saliva, cerebrospinal fluid, or tissue biopsies are inoculated into susceptible cell lines to observe cytopathic effects characteristic of herpesvirus infection. Although viral culture is highly specific, it is time-consuming and less sensitive for latent or low-level infections. Consequently, it has largely been replaced by faster molecular methods in modern diagnostic laboratories.
Polymerase chain reaction (PCR) and real-time PCR are currently the most widely used techniques for herpesvirus detection. These molecular methods identify viral DNA with high sensitivity and specificity, even when viral loads are low. PCR-based assays are particularly valuable for diagnosing infections caused by HSV, CMV, EBV, and VZV. Quantitative PCR also enables measurement of viral load, which is useful for monitoring disease progression and evaluating treatment response, especially in immunocompromised patients and transplant recipients.
Serological testing is another important diagnostic tool used to detect antibodies produced against herpesviruses. Enzyme-linked immunosorbent assay (ELISA), immunofluorescence assays, and Western blot techniques are commonly employed to identify virus-specific immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies. Detection of IgM antibodies generally indicates recent or active infection, whereas IgG antibodies suggest past exposure or latent infection. Serology is especially useful in epidemiological studies and prenatal screening for viruses such as CMV and HSV.
Antigen detection methods, including direct fluorescent antibody tests and immunohistochemistry, can rapidly identify viral proteins in infected tissues or clinical specimens. These methods are useful in acute infections but may have lower sensitivity compared to molecular techniques. In some cases, histopathological examination of infected tissues also provides diagnostic clues, such as multinucleated giant cells and intranuclear inclusion bodies typical of herpesvirus infections.
Advances in molecular diagnostics, including multiplex PCR, next-generation sequencing (NGS), and CRISPR-based assays, are improving the speed and accuracy of herpesvirus detection. These technologies facilitate simultaneous detection of multiple viral pathogens and identification of antiviral resistance mutations. Early and accurate diagnosis remains critical for reducing complications, guiding antiviral therapy, and limiting transmission of Herpesviridae infections.
Treatment of Herpesviridae infections
Treatment of infections caused by the Herpesviridae family primarily involves antiviral therapy aimed at reducing viral replication, alleviating symptoms, preventing complications, and limiting transmission. Although current treatments can effectively control active infections, they generally do not eliminate latent viruses from the body. As a result, herpesvirus infections may reactivate periodically throughout the lifetime of the host.
The most commonly used antiviral agents against herpesviruses are nucleoside analogs, which inhibit viral DNA synthesis. Acyclovir is the prototype antiviral drug widely used for the treatment of HSV and VZV infections. After activation by viral thymidine kinase, acyclovir interferes with viral DNA polymerase activity, thereby preventing viral replication. Related drugs such as valacyclovir and famciclovir possess improved oral bioavailability and are commonly prescribed for recurrent genital herpes, shingles, and mucocutaneous HSV infections.
For severe infections caused by CMV, especially in immunocompromised individuals, antiviral agents such as ganciclovir and valganciclovir are commonly employed. These drugs inhibit CMV DNA polymerase and are effective in managing CMV retinitis, pneumonitis, and systemic infections. In cases of antiviral resistance or drug intolerance, alternative agents such as foscarnet and cidofovir may be used, although their administration is associated with significant nephrotoxicity and other adverse effects.
Supportive treatment also plays an important role in herpesvirus management. Analgesics, antipyretics, hydration, and topical medications may help relieve pain, fever, and skin lesions associated with HSV and VZV infections. In immunocompromised patients, prompt initiation of antiviral therapy is critical to prevent severe complications such as encephalitis, disseminated infection, or organ failure.
Preventive strategies are equally important in controlling herpesvirus infections. Vaccination has proven highly successful against varicella-zoster virus. The varicella vaccine protects against chickenpox, while the recombinant zoster vaccine reduces the risk of shingles and postherpetic neuralgia in older adults. However, effective vaccines for HSV, CMV, and EBV are still under development despite extensive research efforts.
The emergence of antiviral resistance presents a growing challenge in herpesvirus treatment, particularly among patients receiving prolonged therapy. Resistance usually results from mutations in viral thymidine kinase or DNA polymerase genes, reducing drug efficacy. Therefore, continuous monitoring of resistance patterns and development of novel antiviral compounds remain important research priorities.
Recent advances in gene-editing technologies, immunotherapy, and therapeutic vaccines offer promising future approaches for managing herpesvirus infections. Improved understanding of viral latency and immune evasion mechanisms may ultimately lead to curative therapies capable of eliminating persistent infection from the host.
Epidemiology of the Herpesviridae family
The Herpesviridae family comprises globally distributed viruses that infect humans and a wide variety of animal species. These viruses are highly prevalent due to their efficient modes of transmission, lifelong persistence in infected hosts, and ability to establish latent infections with periodic reactivation. Human herpesviruses are widespread across all age groups and populations, with infection rates influenced by geographic location, socioeconomic status, immune status, hygiene practices, and behavioral factors.
Human HSV-1 is one of the most prevalent members of the family, commonly acquired during childhood through oral contact, saliva, or contaminated secretions. In contrast, HSV-2 is primarily sexually transmitted and is more common among sexually active adults. Seroprevalence studies indicate that a significant proportion of the global population carries antibodies against HSV-1 and HSV-2, although many infections remain asymptomatic.
VZV, another alphaherpesvirus, spreads mainly through respiratory droplets and direct contact with skin lesions. Primary infection causes chickenpox, while reactivation later in life leads to herpes zoster (shingles). CMV, a betaherpesvirus, is transmitted through body fluids including saliva, urine, blood, semen, breast milk, and transplanted organs. CMV infection is especially significant in neonates, pregnant women, and immunocompromised individuals such as transplant recipients and patients with HIV/AIDS.
EBV is transmitted primarily through saliva and is strongly associated with infectious mononucleosis and several malignancies, including Burkitt lymphoma and nasopharyngeal carcinoma. Kaposi’s sarcoma-associated herpesvirus (KSHV) is linked to Kaposi’s sarcoma and is more prevalent in immunocompromised populations. Other human herpesviruses, including HHV-6 and HHV-7, are commonly acquired in childhood and are associated with febrile illnesses such as roseola infantum.
Animal herpesviruses also have major veterinary and economic importance. Examples include bovine herpesvirus, equine herpesvirus, pseudorabies virus in swine, and Marek’s disease virus in poultry. These viruses can cause respiratory disease, reproductive failure, neurological disorders, immunosuppression, and neoplastic conditions, leading to substantial economic losses in livestock and poultry industries worldwide.
A major epidemiological feature of herpesviruses is latency. After primary infection, the viruses persist in specific host cells such as neurons, lymphocytes, or glandular tissues without producing active disease. Reactivation may occur due to stress, fever, immunosuppression, hormonal changes, or other triggering factors, resulting in viral shedding and transmission to susceptible hosts. This latent-reactivation cycle contributes significantly to the continued circulation of herpesviruses within populations.
Prevention of Herpesviridae infections
Prevention of herpesvirus infections relies on a combination of personal hygiene measures, vaccination, screening programs, behavioral interventions, and infection-control practices. Because many herpesvirus infections are asymptomatic, prevention can be challenging, particularly in densely populated communities and healthcare settings.
Good personal hygiene, including regular handwashing and avoidance of direct contact with infected lesions or body fluids, is essential for limiting transmission. Individuals with active oral or genital herpes lesions are advised to avoid close physical or sexual contact during symptomatic periods. Safe sexual practices, including condom use and limiting the number of sexual partners, reduce the risk of HSV-2 transmission.
Vaccination represents one of the most effective preventive strategies for certain herpesviruses. The varicella vaccine significantly reduces the incidence of chickenpox, while the herpes zoster vaccine lowers the risk of shingles and postherpetic neuralgia in older adults. In veterinary medicine, vaccines against Marek’s disease virus, bovine herpesvirus, and pseudorabies virus have contributed substantially to disease control in livestock and poultry populations.
In healthcare environments, strict infection-control measures such as sterilization of medical equipment, safe blood transfusion practices, organ donor screening, and isolation precautions are critical for preventing nosocomial transmission. Screening of pregnant women and transplant donors for CMV and other herpesviruses is also important in reducing congenital and opportunistic infections.
Control and management of Herpesviridae infections
Control of herpesvirus infections focuses on reducing disease severity, preventing complications, and minimizing transmission. Antiviral drugs such as acyclovir, valacyclovir, ganciclovir, and famciclovir are widely used to inhibit viral replication and manage both primary and recurrent infections. These drugs are particularly beneficial in immunocompromised patients, where herpesvirus infections can become severe or life-threatening.
Long-term suppressive antiviral therapy may be recommended for individuals with frequent recurrent herpes infections to reduce viral shedding and transmission risk. Early diagnosis through molecular techniques such as polymerase chain reaction (PCR), viral culture, and serological testing improves patient management and outbreak control.
In animal production systems, biosecurity measures including quarantine, sanitation, vaccination, controlled animal movement, and surveillance programs are essential for controlling the spread of herpesvirus-associated diseases. Continuous epidemiological monitoring and research are also important for detecting emerging strains, understanding transmission dynamics, and improving preventive and therapeutic interventions.
References
Acheson N.H (2011). Fundamentals of Molecular Virology. Second edition. John Wiley and Sons Limited, West Sussex, United Kingdom.
Alan J. Cann (2005). Principles of Molecular Virology. 4th edition. Elsevier Academic Press, Burlington, MA, USA.
Alberts B, Bray D, Johnson A, Lewis J, Raff M, Roberts K and Walter P (1998). Essential Cell Biology: An Introduction to the Molecular Biology of the Cell. Third edition. Garland Publishing Inc., New York.
Barrett J.T (1998). Microbiology and Immunology Concepts. Philadelphia, PA: Lippincott-Raven Publishers. USA.
Black, J.G. (2008). Microbiology: Principles and Explorations (7th ed.). Hoboken, NJ: J. Wiley & Sons.
Brian W.J Mahy and Mark H.C van Regenmortel (2010). Desk Encyclopedia of Human and Medical Virology. Elsevier Academic Press, San Diego, USA.
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA.
Cann A.J (2011). Principles of Molecular Virology. Fifth edition. Academic Press, San Diego, United States.
Carter J and Saunders V (2013). Virology: Principles and Applications. Second edition. Wiley-Blackwell, New Jersey, United States.
Champoux J.J, Neidhardt F.C, Drew W.L and Plorde J.J (2004). Sherris Medical Microbiology: An Introduction to Infectious Diseases. 4th edition. McGraw Hill Companies Inc, USA.
Dimmock N (2015). Introduction to Modern Virology. Seventh edition. Wiley-Blackwell, New Jersey, United States.
Dimmock N.J, Easton A.J and Leppard K.N (2001). Introduction to modern virology. 5th edition. Blackwell Science publishers. Oxford, UK.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.