Treponema pallidum (known scientifically as T. pallidum subsp. pallidum) is a Gram variable or Gram-negative, microaerophilic or anaerobic, motile, spiral-shaped bacterium (spirochaete) that is found in the genus Treponema and family Spirochaetaceae. It is the etiologic agent of syphilis, a sexually transmitted disease (STD) in humans. Syphilis is a contagious STD like gonorrhea, and the disease occurs worldwide in both males and females at varying frequency. T. pallidum subsp. pallidum which causes venereal syphilis and congenital syphilis (acquired by the feotus in utero from syphilis infected expectant mothers) is the main important human pathogen in the Treponema genera.
However, other Treponema species that cause significant human infections (e.g. yaws or endemic syphilis caused by T. pallidum subsp. Endemicum amongst others) also exist. Other species of Treponema are usually free-living or commensals and non-pathogenic in nature. They can also be found in the oral cavity of humans (as part of the normal flora of the mucous membranes) and the stomach of animals where they play vital metabolic roles. Leptospira species and Borrelia species are other important spirochaetes that cause significant human infections.
Spirochaetes (which are coiled, helical and actively motile bacteria) normally exists as free-living organisms (or commensals), parasites or important human and animal pathogens. They can be found in mollusks, insects, animals, in the soil and water. T. pallidum subsp. pallidum (which shall be known as T. pallidum in this section)hardly grow outside the human body. This makes in vitro cultivation of the bacteria in the laboratory impossible, and thus hampers further investigations of its metabolic pathways and other significant characteristics.
Current knowledge of the disease mechanism of T. pallidum (which is based on animal model experimentation and some cell culture techniques) is still inefficient in deciphering the full disease process of the organism due to the difficulty associated with its in vitro cultivation.
PATHOGENESIS OF TREPONEMA PALLIDUM INFECTION
Syphilis infection is strictly a human disease that has no animal linkage. T. pallidum gains entry into the human body mainly by direct body contact when there is a break on the skin or epidermis and especially during sexual intercourse with an infected partner (having lesions containing the organism). Ulcerative lesions (containing Treponema pallidum) on the mouth (particularly in those who engage in oral sex), genital organs (penis, cervix or vagina) and the rectum (homosexuals in particular) are usually the main route of transmission of the pathogenic bacteria to susceptible human host.
Direct body contact with the blood or mucosal surfaces of infected persons can also serve as means by which the pathogen is transmitted to susceptible human hosts. Mother to child transmission in utero (i.e. in congenital syphilis) is also possible. Upon invasion, the pathogen migrates to the lymph nodes after multiplying at the portal of entry and then becomes systemic and reaches the bloodstream where it causes bacteraemic conditions in the infected host. The pathogenesis of syphilis infection is complex and thus can be described in a number of steps. Infected untreated individuals usually experience three types or phases of syphilis infection.
PRIMARY SYPHILIS
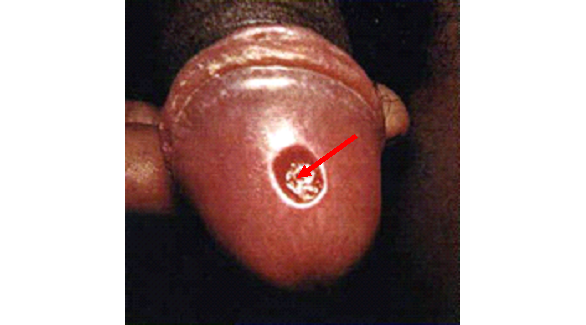
Primary syphilis which is also known as stage I syphilis is characterized by a localized lesion which can occur on the mouth or in the genitalia including the cervix, the vagina and the penis (Figure 1). Chancre or sore due to primary syphilis infection as aforementioned can also be observed on the tongue (Figure 2) and inside or within the walls of the vagina of infected females (Figure 3). This localized lesion which usually forms in about 2 months after initial infection is known as hard chancre. It is painless, and is usually formed at the point of entry of the pathogen (in either the mouth or genital region) as a sore or boil. Primary syphilis usually heals spontaneously without any formal treatment (except in HIV infected persons) but the pathogen disseminates to other vital organs of the body (e.g. CNS and the eyes) via the bloodstream.


SECONDARY SYPHILIS
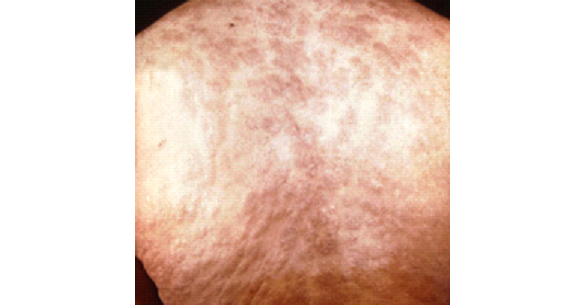
Secondary syphilis or stage II syphilis usually occurs 2-3 months after the self-healing of the primary syphilis. It is characterized by a dissemination of the pathogen in the body of the infected individual. In stage II syphilis, there is a generalized body rash known as maculopapular rash which appears all over the body of the infected individual (Figure 4).
Fever, headache, body pain and malaise are some of the signs and symptoms that are usually associated with this stage of the disease. Secondary syphilis can be asymptomatic with disease progression, and some vital organs of the body such as the liver may be affected. Stage II syphilis like primary syphilis heals spontaneously even without treatment. However, the disease may progress into a latent period during which there are no clinical signs and symptoms of the disease but there is the presence of an infection (which can be proved in the laboratory by serodiagnosis).
Latency or latent period of syphilis infection usually last for about 2 years (for early latency) or 4 years (for late latency), and it later reappears in the individual as tertiary syphilis infection if the immune system of the host fails to clear it from the body. Infected individuals are usually infectious at the early latent period but remain noninfectious at the late latent period of secondary syphilis infection.
TERTIARY SYPHILIS
Tertiary syphilis manifests in many organs of the body as generative lesions generally known as granulomas, gummas or focal lesions. Organs of the body affected in stage III syphilis include the skin, meninges, bone, liver, brain, and the heart amongst others. Stage III syphilis is not infectious and it occurs after many years in some individuals who have secondary syphilis infection. Tertiary syphilis is the result of an untreated syphilis infection, and it can be fatal especially when the CNS is affected resulting in severe neurological disorders amongst other lethal disorders (e.g. aortic aneurysm, loss of sight and dementia). Treponemes can rarely be found in stage III syphilis unlike in stage I and state II where the pathogen can be assayed and identified in the specimens of infected persons.
CONGENITAL SYPHILIS
Congenital syphilisis a non-STD type of syphilis that occurs in the unborn child in which T. pallidum is transmitted from an infected mother to the foetus in utero. Loss of pregnancy or abortion, stillbirth, early birth and the death of the infant are some of the fatalities associated with congenital syphilis infection (which is transplacentally-acquired). Newborns with syphilis infection and who may have survived the disease, usually progress in life with signs and symptoms of the infection and other several anomalies associated with T. pallidum infection in neonates (e.g. blindness, paresis, mental retardation, psychosis et cetera).
LABORATORY DIAGNOSIS OF TREPONEMA PALLIDUM INFECTION
The laboratory diagnosis of syphilis infection is usually based on serodiagnosis and parasite demonstration in stained smears. Biopsy specimens and serum from blood are the samples of choice required for analysis. In vitro cultivation of T. pallidum is still impractical due to the inability of the pathogen to grow outside the human body. Though cell/tissue culture can be used in studying the bacteria pathogen, T. pallidum subculture in tissue culture is not viable.
Motile and corkscrew or spiral-shaped treponemes can be demonstrated in darkfield microscopy from genital lesions (excluding lesions at the oral or anal region) and immunoflourescence microscopy. Note: Lesions at the oral or anal region of syphilis infected individuals should not be examined by darkfield microscopy due to the possibility of a false positive result because some Treponema species are normal flora of these body sites. Several serological tests (e.g. VDRL and RPR) are commercially available for the serological diagnosis of syphilis infection in the laboratory.
IMMUNITY TO TREPONEMA PALLIDUM INFECTION
Re-infection with T. pallidum is possible after a prior infection with the pathogen. Thus protection against syphilis infection is not total as infection occurs again after direct body contact with an infected individual.
TREATMENT OF TREPONEMA PALLIDUM INFECTION
The antibiotic of choice for treating syphilis infection (latent, primary and secondary stage inclusive) is penicillin G which is usually administered extensively and via the parenteral route. Other antibiotics used include cephalosporins, erythromycin and tetracyclines; and these are usually used to treat T. pallidum infected individuals who may be allergic or non-responsive to penicillin G.
PREVENTION AND CONTROL OF TREPONEMA PALLIDUM INFECTION
The primary means of acquiring T. pallidum infection is via sex with an infected person. The only exception is congenital syphilis which is transmitted from an infected mother to the unborn child. Thus, the best way of preventing a syphilis infection is by practicing safe sex, avoiding unsafe sexual practices such as anal sex and oral sex, and by treating any primary infection that occurs.
Infected individuals should ensure that their sex partners are treated as well so as to avoid re-infection. Congenital syphilis can be prevented in neonates by adequate screening and treatment of infected expectant mothers prior to their child delivery. No vaccine currently exists for preventing syphilis infection.
OTHER SUBSPECIES OF TREPONEMA
- T. oralis: T. oralis is a proposed new species of the genus Treponema, and the organism (which is known as an oral spirochaete) has similar morphological and biochemical features with T. denticola. The organismrequires serum for growth, and it produces indole but not ammonia, and propionate and acetate as acid end products.
- T. denticola: T denticola is a Gram-negative, obligate anaerobic, motile and highly proteolytic spirochete bacterium in the genus Treponema. It is abundantly found in the oral cavity of humans; and T. denticola and is highly specialized to survive in this environment. T. denticola is implicated as a causative agent in periodontitis and periodontal diseases in human.
- T. pallidum pertenue: T. p. pertenue is the causative agent of yaws, a tropical infection of the skin, bones and joints of humans. Yaws is spread by direct contact (usually a non-sexual contact) with the fluid from a lesion of an infected person; and the disease is most common among children, who spread it by playing together. Yaw infects only humans.
- T. carateum: T. carateum is the causative agent of the disease known as pinta (which is common in tropical America). It is a spirochete disease that utterly affects the skin of humans.
- T. p. endemicum: T. p. endemicum is the causative agent of bejel or endemic syphilis (treponematosis). Endemic syphilis is a chronic skin and tissue disease exclusively caused by infection by the endemicum subspecies of the spirochete, Treponema pallidum (i.e. T. p. endemicum). Treponematosis, also known as treponemiasis, traditionally refers to the group of non-venereal diseases (including endemic syphilis, a non-venereal syphilis) caused by Treponema species that are morphologically and serologically identical to each other and especially to Treponema pallidum subspecies pallidum, the causative agent of venereal syphilis. The transmission of bejel disease in human population is not venereal in nature even though Treponema pallidum pallidum (the causative agent of venereal syphilis) is morphologically and serologically indistinguishable to Treponema pallidum endemicum (the causative agent of Endemic syphilis).
- T. azotonutricium: T. azotonutricium is commonly found in the gut of termite.
- T. primitia: T. primitia is commonly found in the gut of termite. T. primitia lives in the hindgut of the termite, Zootermopsis angusticolis, and the organism synthesizes acetate – which is the primary source of energy of their insect host. The acetate is mainly synthesized from hydrogen (H2) and carbondioxide (CO2) generated by protozoa (which also inhabit the gut of termites) during the fermentation of wood polysaccharides. Thus, T. primitia is an acetogen – since it can generate acetate. T. primitia is also involved in a mutualistic relationship with both Treponema azotonutricium and the termite in which it resides in.
- T. saccharophilum: T. saccharophilum is a pectinolytic spirochaete commonly isolated from the rumen of bovines including cattle and buffalo. The organism has the ability to breakdown or ferment various polysaccharide including pectin, arabinogalactan, starch, and inulin.
References
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA. Pp. 248-260.
Madigan M.T., Martinko J.M., Dunlap P.V and Clark D.P (2009). Brock Biology of microorganisms. 12th edition. Pearson Benjamin Cummings Publishers. USA. Pp.795-796.
Ryan K, Ray C.G, Ahmed N, Drew W.L and Plorde J (2010). Sherris Medical Microbiology. Fifth edition. McGraw-Hill Publishers, USA.
Prescott L.M., Harley J.P and Klein D.A (2005). Microbiology. 6th ed. McGraw Hill Publishers, USA. Pp. 296-299.
Singleton P and Sainsbury D (1995). Dictionary of microbiology and molecular biology, 3rd ed. New York: John Wiley and Sons.
Talaro, Kathleen P (2005). Foundations in Microbiology. 5th edition. McGraw-Hill Companies Inc., New York, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.