Dental plaque is defined as the tenacious microbial deposit that forms on the hard tissue of the tooth surface. It comprises of living, dead and dying bacteria and their metabolic products as well as the components from the host saliva. Plaque formation also occur on restorations and other prosthetic appliances fixed in individuals who may have lost their teeth or have one dental problem or the other. The term plaque can synonymously be used with biofilm. Dental plaque is the probable cause of dental caries (decay).
Dental plaque cannot be removed by mere washing of the tooth but by the use of tooth brush. Oral bacteria produce several substances inclusive of extracellular polysaccharides (EPS) that promote their adherence or attachment to tooth surfaces. And these molecules contribute to the formation of biofilms on the tooth.
Dental plaque is a major predisposing factor in the development of periodontitis and dental decay. It consists of a mixed community of microbial flora (especially bacteria species) which is enclosed in a matrix that is composed mainly of capsular bacterial polysaccharide molecules such as EPS. Salivary polymers are other components of a dental plaque.
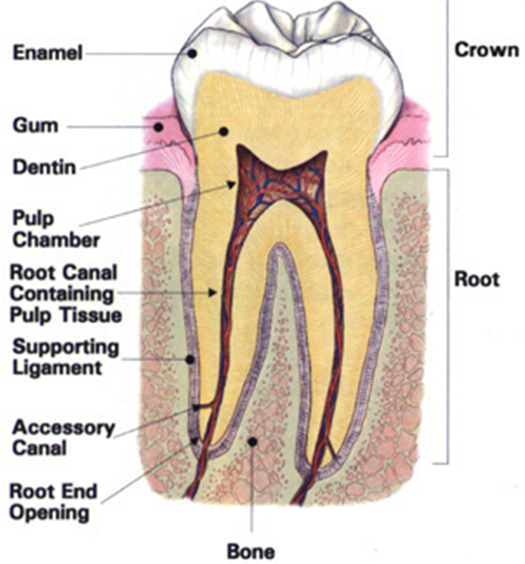
Dental plaque formation on the tooth can be detected by rinsing the mouth with a solution of dye such as erythrosine. This dye is known as a disclosing agent – since it makes the plaque to be visible upon inspection. Disclosing agents are usually given to the affected patients by dentists when they visit the dental clinic for medical checkup (especially as it pertains to tooth examination). Bacterial species in the genus Streptococcus and Neisseria are the early colonizers of the human tooth (especially the surfaces of the enamel); and microbial colonization of the tooth starts immediately after the birth of a child.
As the baby passes through the birth canal of its mother and takes its first breath of life, oral microflora including Streptococcus species begins to build up. Additional bacterial population begins to establish themselves on the surface of the tooth as the child starts to produce its first set of teeth. Once plaque is allowed to build up on the surfaces of the teeth without any sustainable medical intervention to prevent or remove it, the nature of the microorganisms that initially make up the plaque abruptly changes – as other bacterial species including anaerobic bacteria and filamentous bacteria gradually joins the party.
The colonization of the tooth surface by additional microbial flora as aforesaid takes several days to weeks, and they all culminate to the formation of a microcolony of microbes that forms biofilms. Actinomyces viscosus, Veillonella species, Streptococcus mutans and Bacteriodes are the typical examples of microorganisms implicated in the formation of dental plaques in humans.
A summary of the bacteria found in dental plaque formation is shown in Table 1. The site of occurrence of plaque formation on the tooth surface varies. And the nature of plaque formation varies from one site of the tooth to another site on a particular tooth, and they also vary from one individual to another.
Table 1. Bacteria associated with dental plaque formation
| GRAM POSITIVE BACTERIA | GRAM NEGATIVE BACTERIA |
| Streptococcus species | Neisseria species |
| Lactobacillus species | Haemophilus species |
| Corynebacterium species | Veillonella species |
| Actinomycetes | Fusobacterium species |
| Bifidobacterium species | Vibrio species |
| Clostridium species | Spirochetes |
Dental plaque occurs on different parts of the teeth surfaces; both at the anterior part of the tooth (which includes the canine and incisor) and also on the posterior part of the tooth (which include the premolars and molars). Neglect on the part of the individual and not knowing how to clean the teeth properly are some contributing factors to the development of plaque aside microbial activities. Improper brushing of the teeth with good brush leads to the development of pellicles on the tooth surface; and microorganisms get attached to these pellicles to breakdown sugar or carbohydrate molecules.
These pellicles may include glycoproteins, sialic acid, bacterial cell debris, mucins and acidic proline-rich proteins. The carbohydrates are broken down to simple sugars including fructose and glucose – which are utilized by the microbes for metabolic activities. The plaque formed may persist if the individual continues to take food rich in carbohydrates especially those that contain sucrose – the major growth factor for oral bacteria. Oral bacteria utilize the sucrose to increase the amount of organic acids formed; and this increases to a level that inundates the flushing mechanism of the saliva and the neutralizing capacity of the saliva to quell the development.
If left uncontrolled, the plaque (biofilm) formed can reach a density that is very thick and one that harbours several millions of bacterial cells in addition to saliva polymers and food debris. Plaque or biofilm is an excellent platform for the colonization and growth of many bacterial species. In order words, affected individuals require medical intervention to reverse the ugly situation on the tooth surface.
References
Barrett J.T (1998). Microbiology and Immunology Concepts. Philadelphia, PA: Lippincott-Raven Publishers. USA.
Beck, J. D., Slade, G. and Offenbacher, S. (2000). Oral disease, cardiovascular disease and systemic inflammation. Periodontol, 23, 110-20.
Beers M.H., Porter R.S., Jones T.V., Kaplan J.L and Berkwits M (2006). The Merck Manual of Diagnosis and Therapy. Eighteenth edition. Merck & Co., Inc, USA.
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA.
Champoux J.J, Neidhardt F.C, Drew W.L and Plorde J.J (2004). Sherris Medical Microbiology: An Introduction to Infectious Diseases. 4th edition. McGraw Hill Companies Inc, USA.
Davey M.E and O’toole G.A (2000). Microbial biofilms: from ecology to molecular genetics. Microbiol. Mol. Biol. Rev, 64, 847-867.
Gillespie S.H and Bamford K.B (2012). Medical Microbiology and Infection at a glance. 4th edition. Wiley-Blackwell Publishers, UK.
Jenstch, H., Pornowski, R., Kundi, G. and Gocke, R. (2003). Treatment of gingivitis with hyaluronan. J. Clin. Periodontol.,30, 159-164.
Mayooran B, Robin S and John R.T (2000). Dental caries is a preventable infectious disease. Aust. Dent. J, 45, 235-245.
Trahan L.X (1995). A review of its action on mutans streptococci and dental plaque–its clinical significance. Int. Dent. J, 45, 77-92.
Warren L (2008). Review of Medical Microbiology and Immunology. Tenth edition. McGraw Hill Companies Inc, USA.
Wilson B. A, Salyers A.A, Whitt D.D and Winkler M.E (2011). Bacterial Pathogenesis: A molecular Approach. Third edition. American Society of Microbiology Press, USA.
Discover more from Microbiology Class
Subscribe to get the latest posts sent to your email.